Visceral Fat Is a Hormone Problem — Not a Willpower Problem
If you're doing everything right and still carrying stubborn abdominal fat, the problem may not be discipline — it may be your hormones. Learn why visceral fat is a metabolic and hormonal problem, and how we assess and treat it at Precision Hormone Consulting.
If you've cleaned up your diet, started lifting weights, cut back on alcohol, and you're still carrying stubborn fat around your midsection — the frustration is understandable. Most people in that position assume they need to do more, or try harder. What they actually need is better information.
Abdominal fat is not simply the result of caloric excess or insufficient discipline. For a significant portion of people — particularly those in midlife — stubborn visceral fat is a hormonal and metabolic problem. It responds to hormonal and metabolic solutions. Understanding why requires a closer look at what visceral fat actually is.
Not All Body Fat Behaves the Same Way
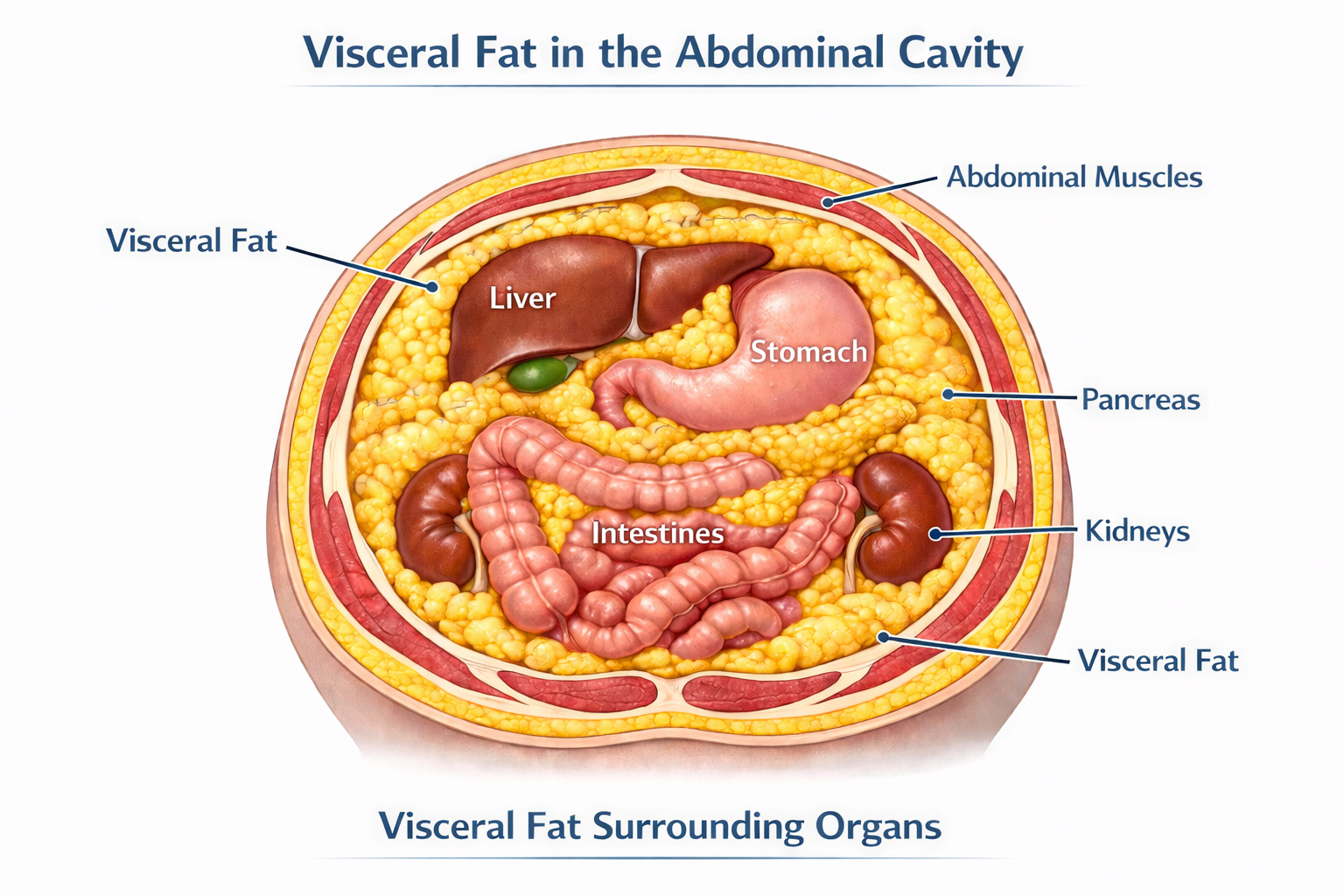
The fat you can pinch just beneath the skin is called subcutaneous fat. It's not metabolically inert, but it's relatively benign compared to the fat that accumulates deep inside the abdominal cavity — surrounding the liver, pancreas, and intestines. That's visceral fat, and it behaves very differently.
Visceral adipose tissue is biologically active. It functions, in many respects, as an endocrine organ — secreting hormones, driving inflammation, and interfering with the metabolic systems that govern energy, appetite, and hormonal balance. The technical term for these secreted compounds is adipokines, and their effects ripple throughout the body.
When visceral fat is elevated, leptin — the hormone that signals satiety — becomes dysregulated, contributing to persistent hunger even in the context of adequate intake. Adiponectin, a hormone that improves insulin sensitivity and reduces inflammation, declines. Pro-inflammatory cytokines like TNF-α and IL-6 rise, creating a state of chronic low-grade systemic inflammation that quietly drives cardiovascular risk, metabolic dysfunction, and hormonal disruption.
Visceral fat is also rich in aromatase — an enzyme that converts androgens like testosterone into estrogens. This is not a minor detail. It means that excess visceral fat doesn't just accumulate as a downstream effect of hormonal imbalance; it actively worsens that imbalance, accelerating androgen breakdown and feeding back on the very hormonal systems that keep fat distribution and metabolism healthy.
Visceral fat doesn't just respond to hormone imbalance — it creates it.
The Hormones Driving Visceral Fat Accumulation
Visceral fat and hormonal dysfunction reinforce each other. Addressing one without the other is rarely sufficient. Here's what the evidence shows for each major hormone axis:
Testosterone
Low testosterone is both a cause and a consequence of visceral fat accumulation. Testosterone promotes lean muscle mass and healthy fat distribution. As levels decline — which happens gradually in both men and women with age — fat preferentially shifts toward the abdomen. That visceral fat then accelerates testosterone breakdown through aromatization, producing more estrogen and suppressing the signaling pathway between the brain and the gonads. The result is a self-reinforcing cycle that worsens over time without intervention.
Estradiol
In women, estradiol plays an underappreciated role in metabolic health. It promotes favorable fat distribution, supports insulin sensitivity, and reduces systemic inflammation. The decline of estradiol at perimenopause and menopause is one of the primary drivers of the visceral fat accumulation many women notice in their 40s and 50s — even without meaningful changes in diet or activity level. Restoring physiologic estradiol is a legitimate metabolic intervention, not merely a quality-of-life measure.
DHEA
DHEA is the most abundant circulating steroid hormone in the body, and it declines significantly with age. Low DHEA correlates with increased visceral adiposity, reduced insulin sensitivity, and an elevated inflammatory state. It receives less attention than testosterone or estradiol in mainstream medicine, but it's a meaningful part of a comprehensive hormonal assessment.
Thyroid — Specifically Free T3
Thyroid hormone drives thermogenesis, fat oxidation, and insulin sensitivity. The clinically relevant form is Free T3 — the metabolically active fraction. Many standard workups stop at TSH, missing patients whose Free T3 is suboptimal even when TSH appears normal. When Free T3 is low, the metabolic engine slows: fat oxidation decreases, insulin resistance worsens, and visceral fat accumulates even in patients doing everything else right.
Cortisol
Visceral adipocytes have a high concentration of glucocorticoid receptors, making them exquisitely responsive to cortisol — the body's primary stress hormone. Chronic psychological or physiological stress translates directly into central fat accumulation, elevated blood glucose, and worsening insulin resistance. Cortisol dysregulation isn't optional to address in any serious approach to metabolic health.
Insulin Resistance
Insulin resistance and visceral fat are so tightly intertwined that separating cause from consequence is often impossible. Visceral fat drives insulin resistance through adipokine dysregulation, chronic inflammation, and excess free fatty acid release into the portal circulation. Insulin resistance, in turn, creates a hormonal environment that favors further visceral fat accumulation. Addressing one without the other rarely produces durable results.
What We Measure — and Why It Matters
Identifying visceral fat burden and its downstream metabolic effects requires looking beyond a scale or a BMI table. BMI, in particular, tells you almost nothing about where fat is distributed or how metabolically active it is. Two people with identical BMIs can carry dramatically different metabolic risk.
At Precision Hormone Consulting, a comprehensive assessment includes:
Waist circumference and waist-to-hip ratio are simple but meaningful starting points — far more predictive of metabolic risk than weight or BMI alone. In-office, we use InBody bioelectrical impedance analysis to go further, generating a validated estimate of visceral fat, lean mass, and body composition that gives us a quantitative baseline and a way to track changes over time. The clinical gold standards for visceral fat measurement — DEXA and MRI — offer greater precision but are expensive and largely inaccessible outside of research settings. For the purposes of clinical monitoring, our combination of anthropometric measures and InBody analysis provides a practical, actionable picture of visceral fat burden without requiring a radiology referral.
Fasting insulin and HOMA-IR — the most direct available measures of insulin resistance. A fasting glucose in the normal range can mask significantly elevated insulin levels, which is where the metabolic damage is already occurring.
Triglyceride/HDL ratio — an accessible and underutilized surrogate for insulin resistance and small, dense LDL particle burden. A standard lipid panel showing normal total cholesterol can coexist with substantial cardiovascular risk in a patient with visceral adiposity and insulin resistance.
hs-CRP — high-sensitivity C-reactive protein, used as a marker of systemic low-grade inflammation driven by visceral fat.
Adiponectin — an inverse marker of visceral fat and insulin resistance. Low levels indicate significant metabolic risk even before glucose dysregulation becomes overt on a standard chemistry panel.
SHBG (Sex Hormone Binding Globulin) — low SHBG is a reliable early signal of hepatic insulin resistance, often appearing before other markers become abnormal. It is particularly useful in women as an early warning sign of metabolic dysfunction.
LH/FSH ratio — in reproductive-age women, normal physiology produces an FSH level approximately twice that of LH. When insulin resistance is present, this ratio begins to narrow — sometimes approaching 1:1 — even before other metabolic markers are overtly abnormal. This is an early, underutilized signal of insulin's effect on the hormonal axis, and it does not require a PCOS diagnosis to be clinically meaningful.
These markers, taken together, provide a far more complete picture of metabolic health than any single value.
The PHC Approach: Treating the Root Cause
A patient came to us in their mid-forties — lean by BMI standards, active, eating well. Their complaint was persistent abdominal fullness and fatigue that had been gradually worsening for two years. Standard labs from their primary care physician had come back normal. Our panel told a different story: suboptimal Free T3, low SHBG, an elevated fasting insulin consistent with early insulin resistance, and a testosterone level that was technically within the reference range but well below what we'd expect for their age and activity level. Within four months of a targeted protocol, their body composition had shifted meaningfully and their energy had returned.
That kind of presentation is common. The tools to identify and address it are available — they just aren't part of routine care.
Hormone Optimization
Restoring physiologic hormone levels is one of the most effective metabolic interventions available. Testosterone optimization in both men and women improves lean muscle mass, reduces visceral fat, and enhances insulin signaling. Estradiol replacement — particularly relevant around perimenopause and menopause — shifts fat distribution favorably and supports metabolic function. DHEA optimization reduces inflammation and supports body composition. Ensuring Free T3 is in an optimal range, not merely a "not flagged" range, restores the metabolic rate that drives fat oxidation.
Peptide Therapy
Growth hormone-releasing peptides are a valuable adjunct for patients with significant visceral fat burden. Tesamorelin has demonstrated specific efficacy in visceral fat reduction in clinical trials. CJC-1295/Ipamorelin combinations support broader growth hormone axis optimization, improving body composition, sleep quality, and recovery.
GLP-1 Medications
For patients with significant metabolic burden or insulin resistance, GLP-1 receptor agonists represent one of the most effective pharmacologic tools currently available. Their mechanisms go well beyond appetite suppression — they improve insulin signaling, reduce hepatic fat, lower systemic inflammation, and produce meaningful, sustained reductions in visceral adiposity.
It's worth noting that GLP-1 is itself a peptide hormone produced naturally in the gut. In patients with metabolic dysfunction, endogenous GLP-1 production is often impaired — meaning these medications are, in a meaningful sense, optimizing a hormone that the body is no longer producing adequately. That framing fits squarely within a hormone optimization model rather than a weight loss drug model.
Lifestyle Integration
No clinical protocol works in isolation. Resistance training, protein-adequate nutrition, quality sleep, and deliberate stress management all independently reduce visceral adiposity and improve insulin sensitivity. Our role is to help patients optimize the full picture — not simply prescribe and monitor. Clinical intervention amplifies the results of good lifestyle fundamentals; it doesn't replace them.
If You've Been Doing the Right Things and Still Not Getting Results
The frustration of doing everything by the book and still carrying stubborn abdominal fat is real — and it usually means something in the hormonal or metabolic picture hasn't been identified yet.
Visceral fat is not a character flaw. It is a metabolic and hormonal problem, and it responds to metabolic and hormonal solutions. The evidence is clear: optimizing testosterone, estradiol, DHEA, thyroid, and metabolic markers produces real, measurable improvements in body composition and long-term health outcomes.
At Precision Hormone Consulting, we specialize in exactly this kind of comprehensive, root-cause evaluation. If you're ready to understand what's actually driving your metabolic health — and address it systematically — we'd be glad to have that conversation.
Schedule a free consultation at precisionhormoneconsulting.com, or call the clinic to book an appointment. Virtual and in-person options are both available.
[DISCLAIMER] This content is for educational purposes only and does not constitute medical advice. Hormone optimization, peptide therapy, and GLP-1 medications involve prescription therapies that require individualized evaluation, monitoring, and ongoing clinical oversight. Some therapies discussed may be used off-label. Results vary. Consult a qualified physician before beginning any new treatment protocol.