Why You Stop Sleeping Deeply After 40 — And What the Growth Hormone Pulse Has to Do With It
Your deep sleep and your growth hormone don't decline separately — they decline together. Here's the mechanism most physicians never explain, and what the data shows about restoring it.
You go to bed. You wake up six hours later. You were technically asleep the whole night — but you don't feel rested. Your joints are stiff. Your mind is slow. Recovery from your workouts has gotten noticeably worse. And nobody has a good explanation.
Here's what most physicians don't connect: deep, restorative sleep and growth hormone secretion are not two separate things. They are the same system — and that system degrades quietly, predictably, starting in your late thirties.
Understanding this mechanism is the first step toward doing something about it.
The Architecture of Sleep — and Where Growth Hormone Lives
Sleep is not a single state. It moves through cycles — typically four to six per night — alternating between lighter stages and a specific phase called slow-wave sleep (SWS), also referred to as Stage 3 or deep NREM sleep. This is the stage characterized by long, rolling delta waves on an EEG. It is the most physically restorative part of the sleep cycle.
Here is what makes slow-wave sleep biologically distinct: it is precisely synchronized with the largest growth hormone pulse of the day.
Within the first 90 minutes after falling asleep, the hypothalamus releases a surge of growth hormone-releasing hormone (GHRH). GHRH activates both the pituitary — triggering GH secretion — and specific sleep-promoting neurons in the preoptic area of the hypothalamus, including the ventrolateral preoptic nucleus (VLPO). These neurons drive slow-wave sleep directly. The result: a single cascade generates both the GH pulse and the deep sleep stage simultaneously.
This is not coincidental overlap. It is bidirectional coupling. More slow-wave sleep produces a larger GH pulse; a larger GH pulse deepens subsequent slow-wave sleep. The two reinforce each other throughout the early part of the night.
That first nocturnal GH pulse often accounts for 50 to 70 percent of the body's total daily growth hormone output. It is not a minor event — it is the primary anabolic signal of the 24-hour cycle.
What Happens to This System as You Age
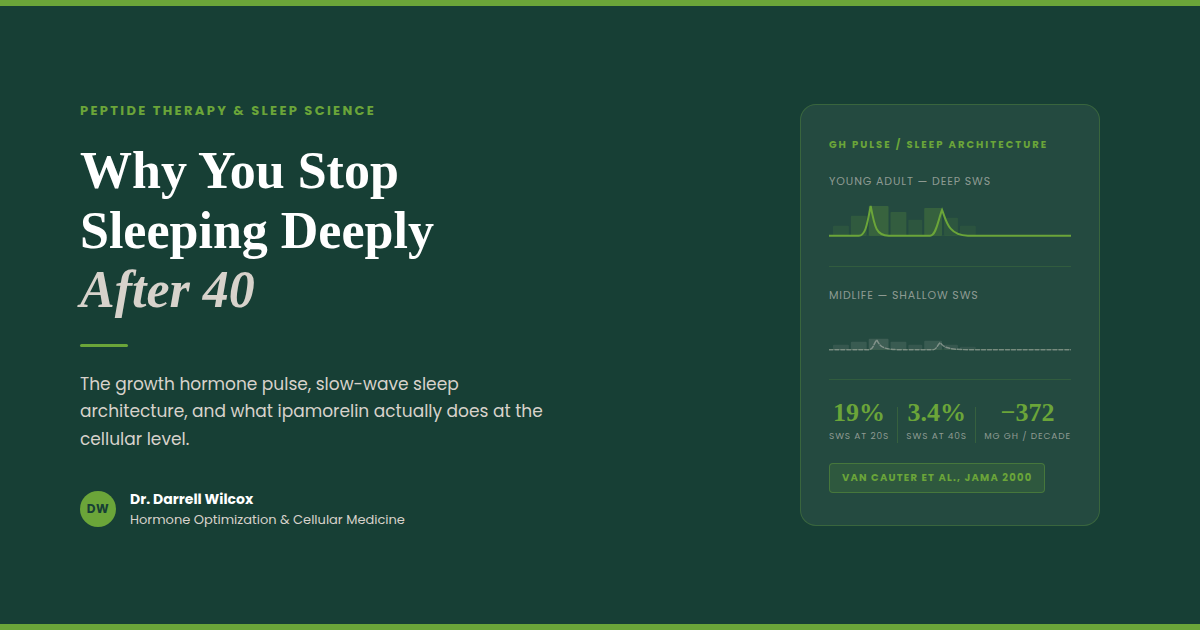
A landmark study published in JAMA tracked sleep architecture and GH secretion across the lifespan in healthy men and found a pattern that is difficult to ignore.
Deep slow-wave sleep accounted for roughly 19 percent of total sleep time in early adulthood. By midlife — ages 36 to 50 — it had dropped to approximately 3.4 percent. Growth hormone secretion tracked that decline almost exactly, falling by more than 370 micrograms per decade from early adulthood through midlife. The association between slow-wave sleep and GH output was statistically significant independent of age: less deep sleep meant less growth hormone, regardless of how old the person was.
This is the somatopause — the gradual age-related decline of the GH axis — playing out at the level of your sleep architecture.
The consequences are clinical. Less GH during sleep means reduced protein synthesis overnight, slower tissue repair, impaired fat metabolism, and diminished recovery from exercise. It also means lighter sleep: the bidirectional loop works in both directions. When GH output drops, slow-wave sleep quality deteriorates further. The system doesn't just decline — it entrains toward a lower equilibrium.
By the time most people notice their sleep has gotten worse and their recovery has slowed down, the mechanism has been shifting for years.
Growth Hormone During Sleep — What It Actually Does
Understanding why sleep-associated GH matters requires a brief look at what growth hormone does downstream.
GH does not act directly on muscle and tissue in most cases. It signals the liver to produce insulin-like growth factor 1 (IGF-1), and it is primarily IGF-1 that drives the anabolic effects most people associate with growth hormone: muscle protein synthesis via the PI3K/Akt/mTOR signaling pathway, satellite cell recruitment for muscle repair, and suppression of protein degradation pathways. GH also acts directly on adipose tissue to promote lipolysis — particularly in visceral fat, which has a high density of GH receptors.
Sleep deprivation disrupts both sides of this equation. Research shows that insufficient or fragmented sleep elevates cortisol while suppressing GH and IGF-1. Cortisol activates muscle protein degradation pathways directly. The net effect is a shift toward a catabolic hormonal environment during the overnight hours — the opposite of what the body is designed to do during sleep.
For someone who trains consistently, the math is straightforward: if the anabolic signaling that drives overnight recovery is compromised, training adaptations slow. Not because of how hard you are working, but because of what is happening — or not happening — during the hours you are not working at all.
Ipamorelin: Restoring the Pulse Without Disrupting the Signal
Ipamorelin is a synthetic pentapeptide that acts as a selective agonist at the ghrelin receptor (GHS-R1a) on the anterior pituitary. It stimulates the pituitary to release growth hormone in a pulsatile pattern — the same physiologic pattern as endogenous GH secretion.
What makes ipamorelin clinically distinct is what it does not do.
Earlier growth hormone-releasing peptides — GHRP-2 and GHRP-6 — also stimulate GH through the ghrelin receptor, but they simultaneously activate non-GHS-R1a pathways that drive elevations in ACTH and cortisol. In a 1998 study that established ipamorelin as a separate category, researchers found that GHRP-2 and GHRP-6 produced significant increases in cortisol and ACTH alongside their GH-releasing effects. Ipamorelin, administered at comparable doses, produced no statistically significant elevation in ACTH or cortisol — even at doses more than 200 times the amount required for maximal GH release. It also had no effect on prolactin, FSH, LH, or TSH.
This selectivity matters clinically. Cortisol is catabolic. A GH secretagogue that raises cortisol alongside GH is working against the recovery environment you are trying to create. Ipamorelin amplifies GH output through the ghrelin receptor while leaving the rest of the hormonal landscape undisturbed.
Administered in the evening, ipamorelin is timed to coincide with the natural nocturnal GH pulse — reinforcing the signal rather than overriding it. The result is an amplified slow-wave sleep-coupled GH release, which supports deeper sleep architecture and enhances the downstream anabolic and tissue repair processes that follow.
Ipamorelin does not introduce synthetic growth hormone. It signals your pituitary to produce more of its own — in the same pulsatile pattern your body was designed to use.
Other Peptides That Work on the Same Axis — and How They Differ
Ipamorelin is one tool in a larger pharmacological toolkit. Other peptides operate on the same GH axis through different receptor pathways, with different clinical profiles.
Sermorelin is a 29-amino-acid analog of GHRH — the upstream signal that the hypothalamus sends to the pituitary to initiate GH release. It is often administered at bedtime to align with the natural nocturnal pulse. Because it works at the GHRH receptor rather than the ghrelin receptor, its GH-releasing effect is subject to somatostatin regulation: when somatostatin levels are high, sermorelin's effect is blunted. It has a relatively short half-life and produces a more transient GH pulse than longer-acting analogs.
Ipamorelin combined with a GHRH analog (such as modified GRF 1-29, sometimes referred to as CJC-1295 without DAC) represents a complementary approach. The GHRH analog activates the GHRH receptor — amplifying the amplitude of each GH pulse. Ipamorelin activates the ghrelin receptor — triggering pulse initiation with high selectivity. These are distinct receptor pathways converging on the same output. A 2006 randomized, placebo-controlled trial confirmed that subcutaneous CJC-1295 produced sustained, dose-dependent increases in GH and IGF-1 in healthy adults, with an estimated half-life of 5.8 to 8.1 days and no serious adverse reactions reported. A companion analysis by Ionescu and Frohman, also in 2006, confirmed that pulsatile GH secretion was preserved throughout continuous GHRH stimulation — GH continued to be released in discrete pulses rather than continuously.
Tesamorelin is a 44-amino-acid GHRH analog with an added structural modification that increases its stability and half-life compared to endogenous GHRH. It is the only peptide in this class that is FDA-approved — specifically for reducing excess visceral abdominal fat in patients with HIV-associated lipodystrophy. Its mechanism is the same GHRH receptor pathway as sermorelin, but with greater potency and duration. In non-HIV populations, it is used off-label for metabolic optimization and body composition. Like sermorelin and CJC-1295, its GH-stimulating effect occurs upstream — it tells the pituitary to release GH rather than supplying GH directly.
The choice among these peptides — and whether they are combined — depends on the individual's GH axis status, metabolic goals, and clinical presentation. No single protocol fits every patient.
What to Expect — Realistic Timeline and Monitoring
Patients who begin ipamorelin-based protocols typically report improvement in sleep quality within two to four weeks — most commonly describing it as feeling more rested after the same hours of sleep, or waking less frequently during the night. Body composition changes, if present, tend to emerge over a longer window of eight to twelve weeks, as improved overnight GH signaling supports changes in fat metabolism and lean tissue preservation.
IGF-1 is the standard monitoring marker. Because these peptides work by amplifying endogenous GH production, IGF-1 rises proportionally. Baseline measurement before initiating therapy, followed by follow-up testing at six to eight weeks, allows for appropriate dose titration and confirms that the GH axis is responding as expected. If IGF-1 rises above age-appropriate reference ranges, dosing should be adjusted.
These peptides are not appropriate for individuals with active malignancy, given the theoretical concern about IGF-1's role in cell proliferation. This is an absolute contraindication. Individual response also varies based on age, baseline GH axis function, sleep quality at the time of initiation, and concurrent hormonal status.
A Note on Regulatory Status
Ipamorelin, sermorelin, and compounded CJC-1295 are not FDA-approved for the indications described here. Their use in adult patients for sleep, recovery, and body composition optimization is off-label. Tesamorelin (Egrifta) carries FDA approval specifically for HIV-associated lipodystrophy; off-label use in other populations requires clinical judgment and informed patient consent.
Compounded versions of these peptides are available through licensed compounding pharmacies and are prescribed by physicians operating within applicable state and federal regulations. Monitoring requirements apply to all protocols.
The Conversation Worth Having
If your sleep has quietly gotten worse over the last several years — if you wake up less rested, recover more slowly, and feel like the work you put in isn't translating the way it used to — the GH axis is worth evaluating.
Conventional medicine rarely looks at this. Sleep is treated as a lifestyle issue. Recovery is treated as a training issue. The hormonal architecture that connects the two is rarely measured and almost never optimized.
That is exactly where this conversation starts.
If you are interested in exploring whether peptide therapy is appropriate for your clinical picture, a virtual consultation is a good first step. We review your history, your symptoms, and where indicated, the relevant labs — and build a protocol around what your physiology actually needs.
Click the link in our bio to connect with us and schedule your free consultation.
[DISCLAIMER]
This post is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Peptide therapies discussed here are used off-label in adults outside of their FDA-approved indications, where applicable. All protocols should be initiated only under the supervision of a licensed physician following individualized clinical evaluation. Individual results vary. IGF-1 monitoring is recommended for patients on GH-axis therapies.
REFERENCES
Van Cauter E, Leproult R, Plat L. Age-Related Changes in Slow Wave Sleep and REM Sleep and Relationship With Growth Hormone and Cortisol Levels in Healthy Men. JAMA. 2000;284(7):861–868. PMID: 10938176
Raun K, Hansen BS, Johansen NL, Thøgersen H, Madsen K, Ankersen M, Andersen PH. Ipamorelin, the first selective growth hormone secretagogue. Eur J Endocrinol. 1998;139(5):552–561. PMID: 9849822
Teichman SL, Neale A, Lawrence B, Gagnon C, Castaigne JP, Frohman LA. Prolonged stimulation of growth hormone (GH) and insulin-like growth factor I secretion by CJC-1295, a long-acting analog of GH-releasing hormone, in healthy adults. J Clin Endocrinol Metab. 2006;91(3):799–805. PMID: 16352683
Ionescu M, Frohman LA. Pulsatile secretion of growth hormone (GH) persists during continuous stimulation by CJC-1295, a long-acting GH-releasing hormone analog. J Clin Endocrinol Metab. 2006;91(12):4792–4797. PMID: 17018654
Weikel JC, Wichniak A, Ising M, Brunner H, Friess E, Held K, Mathias S, Schmid DA, Uhr M, Steiger A. Ghrelin promotes slow-wave sleep in humans. Am J Physiol Endocrinol Metab. 2003;284(2):E407–E415. PMID: 12388174
Yoshida T, Delafontaine P. Mechanisms of IGF-1-mediated regulation of skeletal muscle hypertrophy and atrophy. Cells. 2020;9(9):1970. PMID: 32872179
Chennaoui M et al. How does sleep help recovery from exercise-induced muscle injuries? J Sci Med Sport. 2021;24(10):982–987. PMID: 34074604
Sermorelin vs. Ipamorelin/CJC-1295 vs. Tesamorelin: Which Growth Hormone Peptide Is Right for You?
A physician's guide to the real differences between sermorelin, ipamorelin/CJC-1295, and tesamorelin — three distinct GHRH peptides with different mechanisms, potency, and ideal use cases. Written by Darrell Wilcox, MD.
Growth hormone output declines significantly with age — production can fall by more than half between your 20s and 60s. For many people, that decline shows up as stubborn body fat that won't budge, slower recovery from exercise, poor sleep, and a general sense that the body isn't responding the way it used to.
Peptide therapy is one way to address that decline. But the three most commonly prescribed options — sermorelin, ipamorelin/CJC-1295, and tesamorelin — are not interchangeable versions of the same treatment. Choosing between them should be based on your goals, not whoever marketed their option most aggressively.
What These Peptides Have in Common
None of these are synthetic human growth hormone (HGH). They are growth hormone-releasing hormone analogs that work by signaling your pituitary gland to produce its own GH — naturally, in pulses, through your body's existing feedback loops.
This matters. Synthetic HGH bypasses those feedback mechanisms entirely, which is why it carries risks like insulin resistance and soft tissue overgrowth. These peptides work with your body's regulatory systems, not around them.
All three drive the same downstream process: your pituitary releases GH → your liver produces IGF-1 → IGF-1 drives the benefits you're after: fat metabolism, tissue repair, sleep quality, and body composition improvements. The differences lie in how strongly each peptide stimulates that process, and through what mechanism.
The Three Options
Sermorelin — The Foundation
Sermorelin is the gentlest of the three. It's a fragment of the natural GHRH molecule, has decades of clinical use behind it, and produces a modest, dose-dependent increase in GH output.
Sleep quality is typically the first benefit patients notice, often within two to four weeks. Recovery between training sessions improves. Over three to six months, most patients see gradual improvements in skin elasticity, hair quality, and body composition.
Dosing is simple: one subcutaneous injection daily, typically before bed to align with your body's natural nighttime GH release. Side effects are generally mild — occasional water retention, temporary wrist or hand numbness, minor injection site irritation.
Best for people new to peptide therapy, those with broad wellness goals across sleep, recovery, and gradual body recomposition, and anyone who wants a simple daily protocol with a mild side effect profile.
Ipamorelin/CJC-1295 — The Middle Ground
This is a combination protocol, and the pairing is intentional. CJC-1295 is a GHRH analog that stimulates GH release through the same receptor pathway as sermorelin. Ipamorelin works through a completely different pathway — the ghrelin receptor — and is notable for its selectivity: unlike older secretagogues, it does not significantly raise cortisol or prolactin at therapeutic doses.
Together, they stimulate GH release through two separate mechanisms simultaneously, producing a more robust response than either would alone — and meaningfully stronger than sermorelin. In clinical practice, both are administered as a single combined daily subcutaneous injection, keeping the protocol simple while delivering the synergistic benefit of dual-pathway stimulation.
Sleep and recovery improvements are similar to sermorelin but often more pronounced. Body recomposition is more noticeable. Side effects are moderate — water retention and post-injection flushing are more common than with sermorelin, but cortisol and prolactin remain stable.
Best for patients who want a stronger GH response, those stepping up from sermorelin, and anyone seeking meaningful body recomposition alongside the broader wellness benefits.
Tesamorelin — The High-Intensity Option
Tesamorelin is the full-length GHRH molecule with a structural modification that makes it resistant to the enzyme that normally breaks it down quickly in the body. This gives it a longer duration of action and the most potent GH response of the three.
It is the only peptide in this group with FDA approval — specifically for reducing visceral fat, the dangerous fat that surrounds your internal organs, in a specific patient population. The clinical trials supporting that approval showed IGF-1 increases of 50–100% above baseline and approximately 15% reduction in visceral fat over 26 weeks, confirmed by CT imaging, along with improvements in triglycerides and related metabolic markers.
Dosing is typically daily, though a five-days-on, two-days-off schedule is commonly used in clinical practice to manage water retention. Side effects are the most pronounced of the three — water retention, carpal tunnel-like symptoms from fluid retention, and a small but measurable effect on glucose tolerance in some patients. Monitoring of IGF-1, fasting glucose, and HbA1c is essential throughout treatment.
Best for patients whose primary goal is visceral fat loss, already-fit individuals targeting stubborn midsection fat, and those who want the most aggressive body recomposition results and are prepared for careful monitoring.
A Patient Story
A patient in their late 40s came in frustrated. Consistent training for years, eating well, sleeping reasonably — and still couldn't move the midsection fat or recover the way they used to. Bloodwork was otherwise unremarkable. IGF-1 was in the lower third of the reference range.
We started with ipamorelin/CJC-1295. Within the first month, sleep improved noticeably. By month three, recovery between sessions had shortened and body composition had begun to shift. At six months, they were down several inches at the waist and training harder than they had in a decade.
No shortcuts. The peptide created a more favorable hormonal environment. Consistent training and nutrition did the rest.
How to Choose
Sermorelin is the right starting point if your goals span sleep, recovery, skin, energy, and gradual body composition improvement — or if you're new to injectable peptide therapy and want a gentle introduction. Mildest side effects, simplest daily protocol.
Ipamorelin/CJC-1295 is the step up. Choose this if you want a stronger GH response, more noticeable body recomposition, or if sermorelin didn't deliver the results you were after. Daily combined injection, moderate side effects, dual-pathway stimulation.
Tesamorelin is the high-intensity option. Choose this if visceral fat reduction is your primary goal, you're already doing the lifestyle fundamentals consistently, and you want the most aggressive protocol backed by the strongest clinical evidence. Requires diligent monitoring.
Many patients begin with sermorelin or ipamorelin/CJC-1295 and advance based on their response. Your physician should guide that sequence based on your labs and goals.
What to Expect
Results build progressively. Most patients notice improved sleep and energy within the first two to four weeks. Recovery improvements follow in the first one to three months. Meaningful body composition changes take three to six months of consistent use — don't evaluate results before that three-month mark.
All three protocols require regular monitoring: IGF-1 every three to six months, along with fasting glucose, HbA1c, and thyroid function. These are prescription medications that require physician oversight, not self-directed supplementation.
Ready to Find Out Which Protocol Fits You?
If any of this resonates, the next step is a conversation — not a commitment. At Precision Hormone Consulting, we offer free consultations to review your labs, understand your goals, and determine whether peptide therapy is appropriate and which protocol makes sense for your situation.
You can book a virtual consultation online or call us directly to schedule in person. Either way, you'll leave with a clear picture of where you stand and what your options are.
This article is for educational purposes only and does not constitute medical advice. Growth hormone peptides are prescription medications. Consult a licensed physician before beginning any peptide therapy protocol.