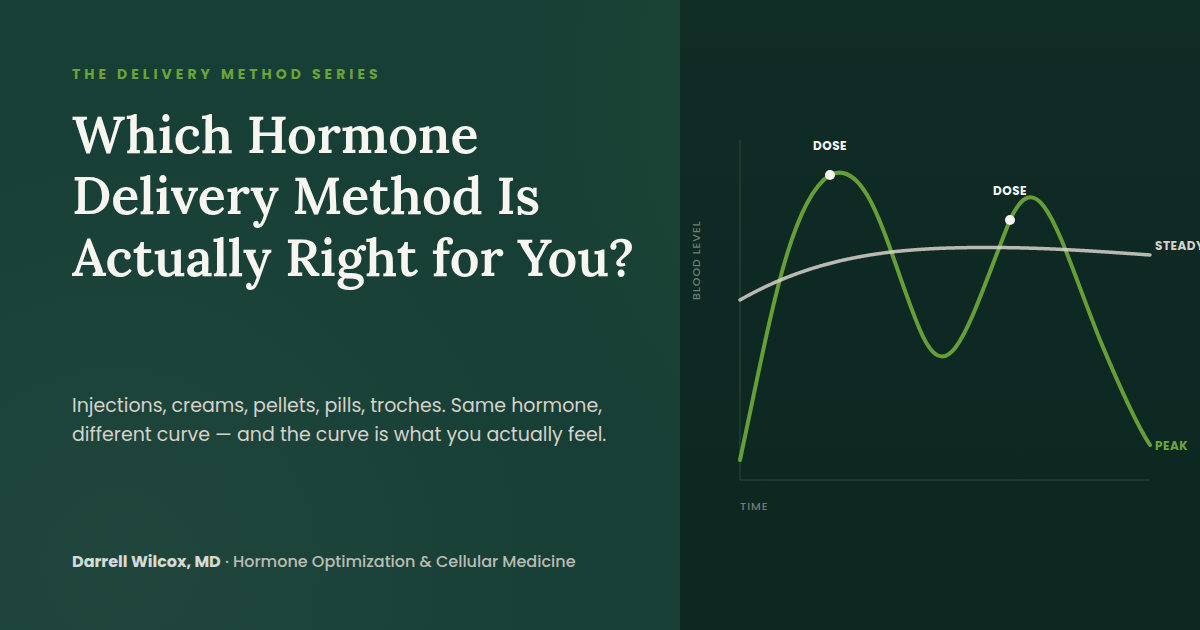
Injections, Creams, Pellets, Pills, Troches: Which Hormone Delivery Method Is Actually Right for You?
Injections, creams, pellets, pills, troches. The delivery method changes how a hormone actually behaves in your body, not just how you take it. Here's the mechanism behind each route, and how to think about which one fits you.
You've finally decided. After months, maybe years, of feeling like a worn-down version of yourself, you're ready to do something about your hormones. And then you start researching, and you hit a wall of options. Injections. Creams. Pellets. Pills. Patches. Troches that dissolve under your tongue. Everyone you talk to has a strong opinion, and somehow every opinion is different.
Here's the part nobody tells you: most of those people aren't wrong. They've just confused what worked for them with what's best for everyone. Those are not the same thing.
The best delivery method isn't a universal answer. It's the one that fits your physiology, your bloodstream, your lifestyle, and your goals.
The delivery method matters more than most people realize, because it determines something the label never quite explains: how the hormone actually behaves once it's in your body. Two people can take the same hormone and have completely different experiences, simply because of how it was delivered. Here's why.
Why Delivery Method Changes Everything
When we talk about hormone delivery, we're really talking about three things. How fast the hormone enters your bloodstream. How steady the level stays. And how predictable that pattern is from person to person.
A hormone that enters quickly and clears quickly produces peaks and valleys. A hormone that enters slowly and steadily produces a flat, stable line. Neither is automatically better. Some people feel their best on a steady line. Others tolerate a gentle rhythm of peaks and troughs just fine, since that's closer to how the body produces hormones on its own.
The trouble starts when a delivery method produces a pattern your body doesn't tolerate well: a peak too high, a trough too low, or a level that swings in a way you feel. That's when people feel off even though they're technically on therapy.
The Three Variables That Actually Matter
Absorption kinetics is how quickly the hormone gets into your system. Half-life is how long it stays before your body clears half of it. Blood-level stability is how flat or how variable the resulting curve is over days or weeks.
Every delivery method is just a different combination of those three variables. Once you understand that, the "which is best" debate mostly dissolves. The better question isn't which method is best. It's which curve fits you.
Testosterone: The Most Debated Delivery Decision
Testosterone has the most delivery options and the loudest opinions, partly because the differences between routes are genuinely large. A comprehensive pharmacokinetic comparison across formulations found that the timing, magnitude, and duration of peak-to-trough testosterone swings vary substantially by route, and that none of the standard formulations actually reproduce the body's natural daily rhythm, where testosterone runs higher in the morning and lower at night.
Intramuscular injections, typically given weekly or every two weeks, create a real peak shortly after the injection and a gradual decline until the next dose. Some people feel great on the peak and flat by the end of the interval. Others feel the swing.
Subcutaneous injections, often given more frequently in smaller doses, tend to produce a gentler, more even curve than intramuscular dosing. A review from the Brigham and Women's men's health research program describes subcutaneous dosing as a safe, practical option with steadier levels between injections than the traditional intramuscular approach, largely because the more frequent, smaller doses smooth out the peak-and-trough pattern.
Topical creams and gels, applied daily, aim for a steadier state but depend heavily on absorption, which varies by skin site. A pharmacokinetic study of testosterone cream applied to scrotal skin found meaningfully faster and higher absorption at that site compared with standard application areas, which is why site matters as much as formulation.
Pellets, inserted under the skin every three to six months, offer real convenience: no daily dosing, no injections to remember. The tradeoff is that once they're in, the dose can't be adjusted. If the level runs too high early on, or too low near the end of the interval, there's no way to correct it until the next insertion.
Troches, which dissolve under the tongue, and nasal gels are less commonly used for testosterone specifically, mainly because absorption through oral mucosa tends to be less consistent from person to person. They're real options some patients specifically ask about, and worth understanding honestly rather than dismissing outright: they can work, but the predictability tends to be lower than injectable or topical routes.
Estradiol and Progesterone: The Same Logic, Different Curves
The delivery conversation isn't unique to testosterone. Estradiol and progesterone follow the same principle: how you take the hormone shapes how it behaves.
Oral estradiol and transdermal estradiol produce strikingly different curves. A pharmacokinetic study comparing a 2 mg oral tablet to a 50 microgram transdermal patch found that oral estradiol spikes to a peak within under an hour and falls off within a few hours, while the patch holds a much steadier, lower level with far less swing. Neither is inherently wrong. Someone who wants convenience and doesn't mind a daily rise and fall may do fine orally. Someone who wants a flatter, more consistent exposure may prefer the patch. Injectable estradiol esters exist as well, following the same peak-then-decline pattern as testosterone injections, just on a different timescale.
Progesterone tells a similar story. Oral micronized progesterone has long been the standard option, and it's well studied precisely because oral progesterone historically had a bioavailability problem: without micronization, very little of it survives the liver's first-pass metabolism intact. Micronization solved enough of that problem to make oral dosing clinically useful, though bioavailability still runs low compared with other routes, which is part of why oral progesterone tends to come with more of the sedating, sleep-related side effect than other forms. Vaginal administration bypasses much of that first-pass effect. A head-to-head pharmacokinetic comparison of two micronized progesterone formulations found that vaginal administration produced meaningfully different absorption and clearance patterns than oral administration of the same drug, underscoring that route, not just dose, drives the outcome. Injectable progesterone exists too, though it's used far less often outside specific clinical contexts, mainly because the other routes usually accomplish the same goal with less discomfort.
What This Looks Like in Practice
A patient in their late forties came in after two years of feeling flat: low energy, a noticeable dip in motivation, and workouts that used to leave them energized now leaving them wiped out for days. An outside provider had started them on a standard weekly intramuscular testosterone injection. The levels on paper looked reasonable, but the patient described feeling great for two or three days after each shot, then increasingly foggy and irritable as the week wore on.
That pattern is not a failure of testosterone therapy. It's a mismatch between the delivery curve and how that particular person's body responds to swings versus steady state. Switching to smaller, more frequent subcutaneous injections smoothed the curve considerably. Within about six weeks, the peak-trough swing the patient had been feeling was largely gone, and the improvement in mood and energy became far more consistent across the week rather than concentrated in the days right after dosing.
Which Route Actually Fits You
There's no universal answer here, and anyone who tells you there is one is selling a preference, not a physiologic fact. A few honest questions help narrow it down. Do you tolerate peaks and troughs well, or do you feel every fluctuation? Do you want the lowest-maintenance option, even if it means less ability to fine-tune once it's started? Are you comfortable with self-injection, or does that rule out an otherwise-reasonable option before you even start?
None of these questions have a wrong answer. They just point toward a different curve.
What to Expect and How Monitoring Works
Whatever route you start with, monitoring is what actually confirms it's working, rather than assuming it is. Initial follow-up labs typically happen around six to eight weeks after starting or changing a protocol, timed to when levels have stabilized for that particular delivery method. After that, monitoring every three to six months is standard once things look settled. This isn't a formality. It's how dose and delivery get fine-tuned to the individual instead of left on a generic starting protocol indefinitely.
Most people notice a shift in energy and mental clarity within four to eight weeks. Changes in body composition and sleep quality tend to take longer, often three to six months, to fully show up. If the first delivery method you try doesn't fit, that's useful information, not a failure. Switching routes is a normal part of finding the right fit, not a sign that hormone therapy itself isn't working for you.
Start with a Conversation
If you're trying to figure out which approach actually fits your body and your life, a free consultation is a reasonable next step. It's a conversation, not a commitment: a chance to ask your questions and understand your options before you decide anything. Because everyone's physiology is genuinely different, that individualized starting point is the whole point. Virtual consultations are available for patients in Texas and Arizona.
This article is for educational purposes only and does not constitute medical advice. It is not intended to diagnose, treat, or recommend any specific therapy, medication, dose, or delivery method. Hormone therapy carries risks and benefits that vary by individual, and some delivery methods or formulations discussed may be used off-label. Always consult a qualified physician before beginning any hormone therapy. Individual results vary.
References
Pastuszak AW, Gittelman M, Tursi JP, Jaffe JS, Schofield D, Miner MM. Pharmacokinetics of testosterone therapies in relation to diurnal variation of serum testosterone levels as men age. Andrology. 2022;10(2):209-222. PMID: 34510812
Figueiredo MG, Gagliano-Jucá T, Basaria S. Testosterone therapy with subcutaneous injections: a safe, practical, and reasonable option. J Clin Endocrinol Metab. 2022;107(3):614-626. PMID: 34698352
Iyer R, Mok SF, Savkovic S, Turner L, Fraser G, Desai R, Jayadev V, Conway AJ, Handelsman DJ. Pharmacokinetics of testosterone cream applied to scrotal skin. Andrology. 2017;5(4):725-731. PMID: 28334510
Setnikar I, Rovati LC, Vens-Cappell B, Hilgenstock C. Pharmacokinetics of estradiol and of estrone during repeated transdermal or oral administration of estradiol. Arzneimittelforschung. 1996;46(8):766-773. PMID: 9125276
Wang H, Liu M, Fu Q, Deng C. Pharmacokinetics of hard micronized progesterone capsules via vaginal or oral route compared with soft micronized capsules in healthy postmenopausal women: a randomized open-label clinical study. Drug Des Devel Ther. 2019;13:2475-2482. PMID: 31440031
Sitruk-Ware R, Bricaire C, De Lignières B, Yaneva H, Mauvais-Jarvis P. Oral micronized progesterone: bioavailability, pharmacokinetics, pharmacological and therapeutic implications. A review. Contraception. 1987;36(4):373-402. PMID: 3327648
Wallace IR, McKinley MC, Bell PM, Hunter SJ. Sex hormone binding globulin and insulin resistance. Clin Endocrinol (Oxf). 2013;78(3):321-329. PMID: 23121642
Laurent MR, Hammond GL, Blokland M, Jardí F, Antonio L, Dubois V, Khalil R, Sterk SS, Gielen E, Decallonne B, Carmeliet G, Kaufman JM, Fiers T, Huhtaniemi IT, Vanderschueren D, Claessens F. Sex hormone-binding globulin regulation of androgen bioactivity in vivo: validation of the free hormone hypothesis. Sci Rep. 2016;6:35539. PMID: 27748448
PROMETRIUM (progesterone, USP) Capsules. Prescribing Information. U.S. Food and Drug Administration, Drugs@FDA, Application No. NDA 020843.
You're Not Losing Muscle Because You Got Lazy
You still train just as hard. So why is the result half what it used to be? The honest answer usually isn't effort. It's a muscle-building signal that quietly fades with age, and a standard lab panel that never measures the part that matters.
You're doing everything right. You still train. You still show up. The weights haven't gotten lighter and your effort hasn't dropped. But somewhere in the last few years, the math stopped working. You put in the same work and get back half the result. Recovery takes longer. The mirror tells a different story than it used to, even though your habits haven't changed.
So you do the thing everyone does. You blame yourself. You decide you've gotten soft, or lazy, or that this is just what getting older feels like. And maybe you went to your doctor, who ran a panel, glanced at it, and told you everything looks normal. You left more confused than when you walked in.
Here's the truth that reframes everything: you're not losing muscle because you got lazy. You're losing it because the signal that builds muscle got quieter, and no amount of effort fully replaces a signal that isn't firing.
What's Actually Happening Inside the Muscle
Muscle isn't built by lifting alone. Lifting creates the demand. What answers that demand is a cascade of biological signals, and testosterone sits near the top of that chain. When testosterone binds to a structure on your muscle cells called the androgen receptor, it switches on a master growth pathway known as mTOR.
Think of mTOR as the muscle's construction foreman. When it's active, it drives protein synthesis, the process that turns the raw material from your diet into new muscle fiber. It also activates satellite cells, the repair crew that rebuilds and reinforces muscle after you train. When the signal is strong, the foreman shows up and the crew gets to work. When the signal weakens, the demand from your training is still there, but fewer workers answer the call.
This is the part conventional advice misses. The research on this is mechanistically clear: testosterone signals through both the androgen receptor and mTOR to produce muscle growth, and when you block either pathway, the growth response falls apart. Effort sets the demand. Hormones determine how much of that demand actually gets met.
The Slow Fade Nobody Warns You About
After about age 35, testosterone in men declines at roughly one to two percent per year. That number sounds small, and at first it is. You don't wake up one morning feeling different. The decline is slow enough that you adapt to it without noticing.
But compound one to two percent over a decade and the gap becomes real. The same workout that built muscle at 35 now barely maintains it at 47. Body composition shifts even when the scale holds steady. Fat creeps in where muscle used to be. And the most frustrating part is that none of this shows up as a dramatic crash. It's a gradual erosion, which is exactly why people blame their own discipline instead of their biology.
The decline is real, measurable, and gradual. That's precisely why it gets mistaken for a personal failing instead of a physiological one.
Why "Normal" Labs Miss the Real Problem
This is where most testosterone testing falls short. When a standard panel checks your testosterone, it usually measures total testosterone, which is everything circulating in your blood. The problem is that most of that testosterone isn't actually available to your muscle cells. It's locked up, bound to a protein called sex hormone-binding globulin, or SHBG.
Only the unbound fraction, called free testosterone, can reach the androgen receptor and switch on the growth signal. And here's the catch that ties the whole story together: SHBG rises as you age. So even if your total testosterone looks respectable on paper, a growing share of it is bound and inactive. The number on your lab report can look fine while the number that actually matters quietly falls.
Two men can walk in with an identical total testosterone of 500. One has low SHBG and plenty of free, available testosterone. The other has high SHBG, and functionally his muscles are working with the testosterone of a man at half that number. Same lab value. Completely different biology. If your panel only measured total testosterone, you'd never know which man you are.
This is the difference between a result that's technically normal and a result that's actually optimal for how you feel and function. The reference range tells you that you fall within the broad population spread. It doesn't tell you whether your biology is doing what you need it to do.
What the Evidence Shows
The relationship between available testosterone and muscle isn't a clinical hunch. In a controlled dose-response trial, researchers gave healthy men carefully graded doses of testosterone and measured the result. Muscle mass and strength increased in direct proportion to the dose. More available testosterone meant more muscle, in a clean, dose-dependent line. This is direct evidence that the amount of testosterone reaching your tissue isn't a minor detail. It's a primary lever on how much muscle you can hold.
Pair that with the mechanistic work showing testosterone driving muscle growth through the androgen receptor and mTOR, and the picture is complete. The signal builds the muscle. The strength of the signal determines the outcome. When the signal fades with age and gets further muted by rising SHBG, the result you see in the mirror is not a character flaw. It's biology following its own rules.
A Patient You Might Recognize
Consider a composite picture drawn from patterns I see often. A patient in their early fifties comes in frustrated. They've trained consistently for years. Over the last two or three years, despite no change in effort, they've watched strength plateau and slowly slip, while a layer of fat settled in that wasn't there before. Their previous doctor ran a testosterone panel, saw a total number inside the reference range, and sent them on their way with a shrug.
When we look closer, the total testosterone is indeed mid-range. But the free testosterone is low, and SHBG is elevated. The available signal is far weaker than the headline number suggested. Nothing about this person's discipline was the problem. The standard panel simply never measured the thing that mattered.
What This Means for You
If you've been blaming yourself for a body that stopped responding, it's worth stepping back and asking whether the real issue was ever effort at all. The honest path forward starts with measuring the right things. That means looking beyond total testosterone to free testosterone, SHBG, and the broader hormonal picture, so you understand what your muscle cells are actually working with.
It's worth being clear-eyed here. Hormone optimization isn't a shortcut, and it isn't for everyone. It requires proper evaluation, ongoing monitoring, and an honest conversation about benefits, individual variability, and what the data does and doesn't support. The point isn't to chase a number. The point is to restore a signal that's been quietly fading, so the work you're already putting in finally produces the result it should.
You were never lazy. The signal got quiet. The work starts with finding out by exactly how much.
Let's Talk
If this sounds like your experience, you don't have to keep guessing. A free consultation is a straightforward conversation about your symptoms, your goals, and whether a deeper look at your hormones makes sense for you. It's bookable virtually, on your schedule. No pressure, no commitment, just a chance to finally get answers that the standard panel never gave you.
This content is for educational purposes only and does not constitute medical advice. It is not intended to diagnose, treat, cure, or prevent any disease. Hormone therapy involves potential risks and benefits that vary by individual and requires evaluation and ongoing monitoring by a qualified physician. Some therapies discussed may involve off-label use. Always consult a licensed healthcare provider before making decisions about your health.
References
Basualto-Alarcón C, Jorquera G, Altamirano F, Jaimovich E, Estrada M. Testosterone signals through mTOR and androgen receptor to induce muscle hypertrophy. Med Sci Sports Exerc. 2013;45(9):1712-1720. PMID: 23470307
Bhasin S, Woodhouse L, Casaburi R, et al. Testosterone dose-response relationships in healthy young men. Am J Physiol Endocrinol Metab. 2001;281(6):E1172-E1181. PMID: 11701431

Progesterone Is Being Prescribed to Men. Here's Why That's a Problem.
The same compound class used clinically to suppress male sexual function is being prescribed by some providers for hormone "balance." Here's what the data actually shows.
Some men on hormone therapy aren't getting better. Their energy is flat. Their libido is low. Their labs look reasonable on paper. But they don't feel optimized — and when you look at their protocol, one thing stands out.
Progesterone.
It's in more male protocols than it should be. Some providers include it for "balance." Some offer it as a sleep aid. The intentions may be reasonable. The biology is not.
Progesterone is a powerful hormone. In female physiology, it's essential — stabilizing, protective, deeply beneficial. But the female body evolved to receive it. The male body did not. And the research on what progesterone actually does inside a man makes that distinction impossible to ignore.
Problem 1: Progesterone Drives Inflammation in Men
Start with the data.
A 2005 study published in the Journal of Clinical Endocrinology & Metabolism examined the relationship between progesterone and inflammation in healthy men — not sick men, not men on medications. Healthy men, aged 20 to 50.
In the first arm, researchers measured endogenous progesterone levels and compared them against a panel of inflammation markers. The findings were unambiguous. Higher progesterone tracked directly with elevated IL-6, C-reactive protein, VCAM-1, E-selectin, and neutrophil counts. Every marker moved in the wrong direction as progesterone rose.
The second arm was a controlled trial. Men who received an exogenous progestin alongside testosterone saw IL-6 spike sharply. Anti-inflammatory IL-10 — the body's counter-regulatory response — dropped significantly. Men receiving testosterone alone showed the opposite: their inflammatory profile improved.
The authors concluded directly: progesterone corresponds to an inflammatory profile in healthy men, and exogenous progestins amplify that effect.
This is not a theoretical concern. IL-6 and CRP are not obscure research endpoints. They are markers of systemic inflammation — the same inflammatory burden that drives cardiovascular disease, metabolic dysfunction, insulin resistance, and accelerated biological aging. A protocol increasing that burden isn't optimizing anything. It is working against the very outcomes it claims to support.
Problem 2: Progestins Tell the Male Hormonal Axis to Shut Down
The second problem runs deeper.
Progestins suppress LH and FSH — the gonadotropins that drive endogenous testosterone production. This isn't a side effect. It's a primary pharmacological mechanism. It's exactly why progestins have been studied for decades in male hormonal contraception research: combined with testosterone, they drive pituitary output toward zero and shut down spermatogenesis. This has been demonstrated in clinical trials, published in peer-reviewed literature, and replicated across multiple progestin compounds.
What this means in the context of hormone optimization: adding a progestogen to a male protocol means adding a compound that pharmacologically signals the hypothalamic-pituitary axis to stand down. Less LH. Less FSH. Less endogenous testosterone stimulus.
A man on exogenous testosterone may not feel this acutely — his levels are being replaced. But the axis-level interference doesn't disappear. You are running an optimization protocol with one hand while using the other to suppress the system that protocol depends on.
There is no legitimate optimization rationale for this in men.
Problem 3: This Is the Same Compound Class Used to Eliminate Male Sexual Function
Here is what makes the clinical picture impossible to rationalize.
Progestogens — specifically medroxyprogesterone acetate — are used clinically in the management of male sex offenders. The therapeutic goal is the deliberate suppression of male sexual function. The published literature documents the effects with precision: reduced libido, diminished erectile capacity, decreased sexual arousal, blunted drive.
That is not a side effect. That is the intended mechanism. It is the reason it works for that purpose.
Now consider the population walking into hormone optimization clinics. Men presenting with low libido. Men with erectile dysfunction. Men who feel flat, disengaged, sexually underperforming. These are the exact symptoms that bring people through the door.
And some of those men are being given a compound class whose documented mechanism in male physiology is the suppression of exactly those functions.
That's not an overstatement. It is a direct reading of the published clinical literature. The compound being offered as part of the solution shares a mechanism with drugs used deliberately to eliminate male sexual function.
Why the Confusion Persists
Progesterone has a genuinely impressive clinical profile — in women.
Better sleep. Cardiovascular protection. Mood stability. Endometrial balance. The evidence base in female BHRT is strong. The benefits are real.
The error is transferring that profile across a physiological boundary where it doesn't apply. Steroid hormones don't work the same way in every body. The response depends entirely on the cellular environment receiving the signal: which receptors are expressed, how they're wired, what downstream pathways activate.
Men and women do not run the same hormonal operating system. Progesterone belongs in female physiology. The data on what it does in male physiology — inflammation, gonadotropin suppression, sexual dysfunction — is not ambiguous.
What I See in Practice
When a man comes in not responding to what should be a well-constructed protocol, progesterone is one of the first things I look at.
The presentation is often subtle. Energy that should be better by now. Sleep that hasn't improved the way it should. Libido that isn't where it needs to be. Inflammatory markers on labs that don't have a clean explanation.
Consider a patient in his mid-50s: active, otherwise healthy, two years into testosterone therapy. Testosterone levels optimized. Thyroid addressed. CRP still elevated. Energy inconsistent. His prior protocol included progesterone — added by a previous provider for sleep support.
Removing the progesterone and restructuring the protocol around compounds appropriate for male physiology: CRP normalized. Sleep improved. Energy stabilized. Nothing dramatic was added. Something that didn't belong was removed.
That is frequently how optimization actually works. It isn't always about adding more. It's about identifying what's creating friction and eliminating it.
What Belongs in a Male Hormone Protocol
A well-constructed male protocol is built around what the male endocrine system is designed to use.
Testosterone optimization — not just reaching a reference range, but achieving the balance of free testosterone, total testosterone, estradiol, and SHBG that produces genuine clinical results.
Thyroid — not just TSH, but Free T3, Free T4, and the conversion pathway where the clinically meaningful information actually lives.
DHEA-S and pregnenolone — compounds the male adrenal and neurological systems are equipped to use effectively, frequently low in men presenting with fatigue and cognitive decline.
Progesterone is not on that list. Not because it was overlooked. Because the male endocrine system wasn't built to use it — and three separate lines of clinical evidence explain what happens when it tries.
The same compound class used clinically to suppress male sexual function is appearing in male hormone optimization protocols. That gap between what the data shows and what some providers prescribe is exactly where patient outcomes get lost.
Is Your Protocol Actually Built for You?
If you're on a hormone protocol that includes progesterone and you haven't felt optimized, that's worth examining — not as a coincidence, but as a mechanism.
A thorough evaluation looks at the full panel: free testosterone, SHBG, estradiol, thyroid function, DHEA-S, cortisol, and inflammatory markers. From there, the goal is a protocol built around what your physiology is designed to use.
Virtual consultations are available and the first conversation is free. Bring your labs if you have them. The goal is a straight answer about whether your protocol is actually working for you — or against you.
References
Zitzmann M, Erren M, Kamischke A, Simoni M, Nieschlag E. Endogenous progesterone and the exogenous progestin norethisterone enanthate are associated with a proinflammatory profile in healthy men. J Clin Endocrinol Metab. 2005 Dec;90(12):6603–8. — PMID: 16204370
Handelsman DJ, Conway AJ, Howe CJ, Turner L, Mackey MA. Establishing the minimum effective dose and additive effects of depot progestin in suppression of human spermatogenesis by a testosterone depot. J Clin Endocrinol Metab. 1996 Nov;81(11):4113–21. — PMID: 8923869
Cooper AJ. Progestogens in the treatment of male sex offenders: a review. Can J Psychiatry. 1986 Feb;31(1):73–9. — PMID: 2936441
[DISCLAIMER]
This content is for educational purposes only and does not constitute medical advice. Hormone therapy involves individualized clinical evaluation and is not appropriate for everyone. Always consult a qualified healthcare provider before starting, stopping, or modifying any hormone protocol.
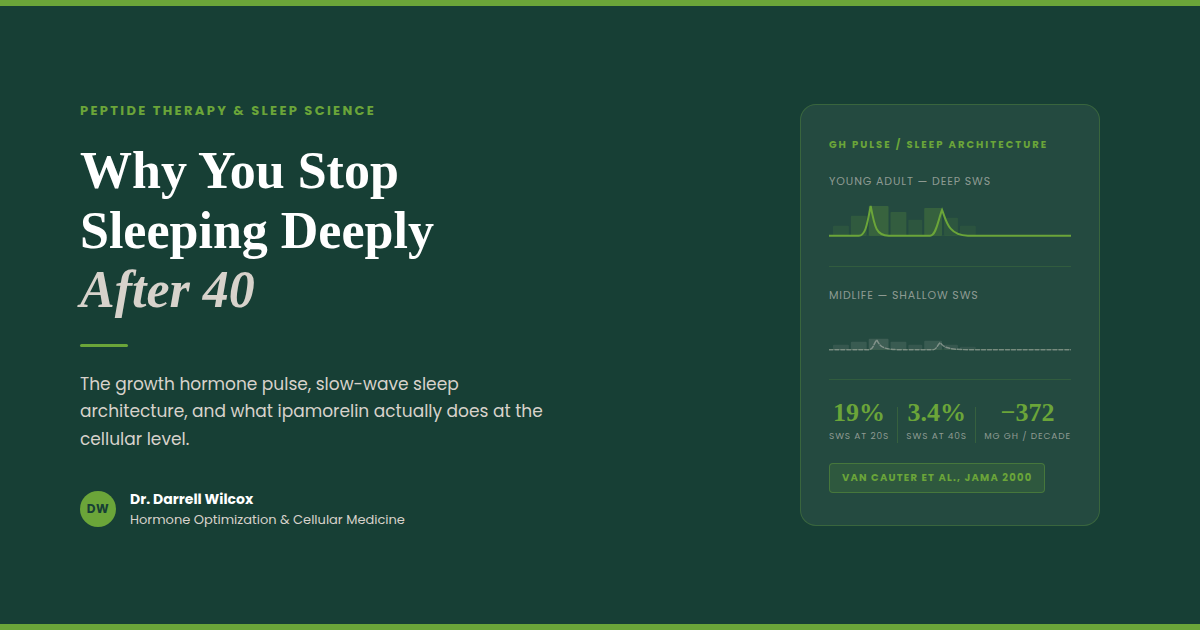
Why You Stop Sleeping Deeply After 40 — And What the Growth Hormone Pulse Has to Do With It
Your deep sleep and your growth hormone don't decline separately — they decline together. Here's the mechanism most physicians never explain, and what the data shows about restoring it.
You go to bed. You wake up six hours later. You were technically asleep the whole night — but you don't feel rested. Your joints are stiff. Your mind is slow. Recovery from your workouts has gotten noticeably worse. And nobody has a good explanation.
Here's what most physicians don't connect: deep, restorative sleep and growth hormone secretion are not two separate things. They are the same system — and that system degrades quietly, predictably, starting in your late thirties.
Understanding this mechanism is the first step toward doing something about it.
The Architecture of Sleep — and Where Growth Hormone Lives
Sleep is not a single state. It moves through cycles — typically four to six per night — alternating between lighter stages and a specific phase called slow-wave sleep (SWS), also referred to as Stage 3 or deep NREM sleep. This is the stage characterized by long, rolling delta waves on an EEG. It is the most physically restorative part of the sleep cycle.
Here is what makes slow-wave sleep biologically distinct: it is precisely synchronized with the largest growth hormone pulse of the day.
Within the first 90 minutes after falling asleep, the hypothalamus releases a surge of growth hormone-releasing hormone (GHRH). GHRH activates both the pituitary — triggering GH secretion — and specific sleep-promoting neurons in the preoptic area of the hypothalamus, including the ventrolateral preoptic nucleus (VLPO). These neurons drive slow-wave sleep directly. The result: a single cascade generates both the GH pulse and the deep sleep stage simultaneously.
This is not coincidental overlap. It is bidirectional coupling. More slow-wave sleep produces a larger GH pulse; a larger GH pulse deepens subsequent slow-wave sleep. The two reinforce each other throughout the early part of the night.
That first nocturnal GH pulse often accounts for 50 to 70 percent of the body's total daily growth hormone output. It is not a minor event — it is the primary anabolic signal of the 24-hour cycle.
What Happens to This System as You Age
A landmark study published in JAMA tracked sleep architecture and GH secretion across the lifespan in healthy men and found a pattern that is difficult to ignore.
Deep slow-wave sleep accounted for roughly 19 percent of total sleep time in early adulthood. By midlife — ages 36 to 50 — it had dropped to approximately 3.4 percent. Growth hormone secretion tracked that decline almost exactly, falling by more than 370 micrograms per decade from early adulthood through midlife. The association between slow-wave sleep and GH output was statistically significant independent of age: less deep sleep meant less growth hormone, regardless of how old the person was.
This is the somatopause — the gradual age-related decline of the GH axis — playing out at the level of your sleep architecture.
The consequences are clinical. Less GH during sleep means reduced protein synthesis overnight, slower tissue repair, impaired fat metabolism, and diminished recovery from exercise. It also means lighter sleep: the bidirectional loop works in both directions. When GH output drops, slow-wave sleep quality deteriorates further. The system doesn't just decline — it entrains toward a lower equilibrium.
By the time most people notice their sleep has gotten worse and their recovery has slowed down, the mechanism has been shifting for years.
Growth Hormone During Sleep — What It Actually Does
Understanding why sleep-associated GH matters requires a brief look at what growth hormone does downstream.
GH does not act directly on muscle and tissue in most cases. It signals the liver to produce insulin-like growth factor 1 (IGF-1), and it is primarily IGF-1 that drives the anabolic effects most people associate with growth hormone: muscle protein synthesis via the PI3K/Akt/mTOR signaling pathway, satellite cell recruitment for muscle repair, and suppression of protein degradation pathways. GH also acts directly on adipose tissue to promote lipolysis — particularly in visceral fat, which has a high density of GH receptors.
Sleep deprivation disrupts both sides of this equation. Research shows that insufficient or fragmented sleep elevates cortisol while suppressing GH and IGF-1. Cortisol activates muscle protein degradation pathways directly. The net effect is a shift toward a catabolic hormonal environment during the overnight hours — the opposite of what the body is designed to do during sleep.
For someone who trains consistently, the math is straightforward: if the anabolic signaling that drives overnight recovery is compromised, training adaptations slow. Not because of how hard you are working, but because of what is happening — or not happening — during the hours you are not working at all.
Ipamorelin: Restoring the Pulse Without Disrupting the Signal
Ipamorelin is a synthetic pentapeptide that acts as a selective agonist at the ghrelin receptor (GHS-R1a) on the anterior pituitary. It stimulates the pituitary to release growth hormone in a pulsatile pattern — the same physiologic pattern as endogenous GH secretion.
What makes ipamorelin clinically distinct is what it does not do.
Earlier growth hormone-releasing peptides — GHRP-2 and GHRP-6 — also stimulate GH through the ghrelin receptor, but they simultaneously activate non-GHS-R1a pathways that drive elevations in ACTH and cortisol. In a 1998 study that established ipamorelin as a separate category, researchers found that GHRP-2 and GHRP-6 produced significant increases in cortisol and ACTH alongside their GH-releasing effects. Ipamorelin, administered at comparable doses, produced no statistically significant elevation in ACTH or cortisol — even at doses more than 200 times the amount required for maximal GH release. It also had no effect on prolactin, FSH, LH, or TSH.
This selectivity matters clinically. Cortisol is catabolic. A GH secretagogue that raises cortisol alongside GH is working against the recovery environment you are trying to create. Ipamorelin amplifies GH output through the ghrelin receptor while leaving the rest of the hormonal landscape undisturbed.
Administered in the evening, ipamorelin is timed to coincide with the natural nocturnal GH pulse — reinforcing the signal rather than overriding it. The result is an amplified slow-wave sleep-coupled GH release, which supports deeper sleep architecture and enhances the downstream anabolic and tissue repair processes that follow.
Ipamorelin does not introduce synthetic growth hormone. It signals your pituitary to produce more of its own — in the same pulsatile pattern your body was designed to use.
Other Peptides That Work on the Same Axis — and How They Differ
Ipamorelin is one tool in a larger pharmacological toolkit. Other peptides operate on the same GH axis through different receptor pathways, with different clinical profiles.
Sermorelin is a 29-amino-acid analog of GHRH — the upstream signal that the hypothalamus sends to the pituitary to initiate GH release. It is often administered at bedtime to align with the natural nocturnal pulse. Because it works at the GHRH receptor rather than the ghrelin receptor, its GH-releasing effect is subject to somatostatin regulation: when somatostatin levels are high, sermorelin's effect is blunted. It has a relatively short half-life and produces a more transient GH pulse than longer-acting analogs.
Ipamorelin combined with a GHRH analog (such as modified GRF 1-29, sometimes referred to as CJC-1295 without DAC) represents a complementary approach. The GHRH analog activates the GHRH receptor — amplifying the amplitude of each GH pulse. Ipamorelin activates the ghrelin receptor — triggering pulse initiation with high selectivity. These are distinct receptor pathways converging on the same output. A 2006 randomized, placebo-controlled trial confirmed that subcutaneous CJC-1295 produced sustained, dose-dependent increases in GH and IGF-1 in healthy adults, with an estimated half-life of 5.8 to 8.1 days and no serious adverse reactions reported. A companion analysis by Ionescu and Frohman, also in 2006, confirmed that pulsatile GH secretion was preserved throughout continuous GHRH stimulation — GH continued to be released in discrete pulses rather than continuously.
Tesamorelin is a 44-amino-acid GHRH analog with an added structural modification that increases its stability and half-life compared to endogenous GHRH. It is the only peptide in this class that is FDA-approved — specifically for reducing excess visceral abdominal fat in patients with HIV-associated lipodystrophy. Its mechanism is the same GHRH receptor pathway as sermorelin, but with greater potency and duration. In non-HIV populations, it is used off-label for metabolic optimization and body composition. Like sermorelin and CJC-1295, its GH-stimulating effect occurs upstream — it tells the pituitary to release GH rather than supplying GH directly.
The choice among these peptides — and whether they are combined — depends on the individual's GH axis status, metabolic goals, and clinical presentation. No single protocol fits every patient.
What to Expect — Realistic Timeline and Monitoring
Patients who begin ipamorelin-based protocols typically report improvement in sleep quality within two to four weeks — most commonly describing it as feeling more rested after the same hours of sleep, or waking less frequently during the night. Body composition changes, if present, tend to emerge over a longer window of eight to twelve weeks, as improved overnight GH signaling supports changes in fat metabolism and lean tissue preservation.
IGF-1 is the standard monitoring marker. Because these peptides work by amplifying endogenous GH production, IGF-1 rises proportionally. Baseline measurement before initiating therapy, followed by follow-up testing at six to eight weeks, allows for appropriate dose titration and confirms that the GH axis is responding as expected. If IGF-1 rises above age-appropriate reference ranges, dosing should be adjusted.
These peptides are not appropriate for individuals with active malignancy, given the theoretical concern about IGF-1's role in cell proliferation. This is an absolute contraindication. Individual response also varies based on age, baseline GH axis function, sleep quality at the time of initiation, and concurrent hormonal status.
A Note on Regulatory Status
Ipamorelin, sermorelin, and compounded CJC-1295 are not FDA-approved for the indications described here. Their use in adult patients for sleep, recovery, and body composition optimization is off-label. Tesamorelin (Egrifta) carries FDA approval specifically for HIV-associated lipodystrophy; off-label use in other populations requires clinical judgment and informed patient consent.
Compounded versions of these peptides are available through licensed compounding pharmacies and are prescribed by physicians operating within applicable state and federal regulations. Monitoring requirements apply to all protocols.
The Conversation Worth Having
If your sleep has quietly gotten worse over the last several years — if you wake up less rested, recover more slowly, and feel like the work you put in isn't translating the way it used to — the GH axis is worth evaluating.
Conventional medicine rarely looks at this. Sleep is treated as a lifestyle issue. Recovery is treated as a training issue. The hormonal architecture that connects the two is rarely measured and almost never optimized.
That is exactly where this conversation starts.
If you are interested in exploring whether peptide therapy is appropriate for your clinical picture, a virtual consultation is a good first step. We review your history, your symptoms, and where indicated, the relevant labs — and build a protocol around what your physiology actually needs.
Click the link in our bio to connect with us and schedule your free consultation.
[DISCLAIMER]
This post is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Peptide therapies discussed here are used off-label in adults outside of their FDA-approved indications, where applicable. All protocols should be initiated only under the supervision of a licensed physician following individualized clinical evaluation. Individual results vary. IGF-1 monitoring is recommended for patients on GH-axis therapies.
REFERENCES
Van Cauter E, Leproult R, Plat L. Age-Related Changes in Slow Wave Sleep and REM Sleep and Relationship With Growth Hormone and Cortisol Levels in Healthy Men. JAMA. 2000;284(7):861–868. PMID: 10938176
Raun K, Hansen BS, Johansen NL, Thøgersen H, Madsen K, Ankersen M, Andersen PH. Ipamorelin, the first selective growth hormone secretagogue. Eur J Endocrinol. 1998;139(5):552–561. PMID: 9849822
Teichman SL, Neale A, Lawrence B, Gagnon C, Castaigne JP, Frohman LA. Prolonged stimulation of growth hormone (GH) and insulin-like growth factor I secretion by CJC-1295, a long-acting analog of GH-releasing hormone, in healthy adults. J Clin Endocrinol Metab. 2006;91(3):799–805. PMID: 16352683
Ionescu M, Frohman LA. Pulsatile secretion of growth hormone (GH) persists during continuous stimulation by CJC-1295, a long-acting GH-releasing hormone analog. J Clin Endocrinol Metab. 2006;91(12):4792–4797. PMID: 17018654
Weikel JC, Wichniak A, Ising M, Brunner H, Friess E, Held K, Mathias S, Schmid DA, Uhr M, Steiger A. Ghrelin promotes slow-wave sleep in humans. Am J Physiol Endocrinol Metab. 2003;284(2):E407–E415. PMID: 12388174
Yoshida T, Delafontaine P. Mechanisms of IGF-1-mediated regulation of skeletal muscle hypertrophy and atrophy. Cells. 2020;9(9):1970. PMID: 32872179
Chennaoui M et al. How does sleep help recovery from exercise-induced muscle injuries? J Sci Med Sport. 2021;24(10):982–987. PMID: 34074604
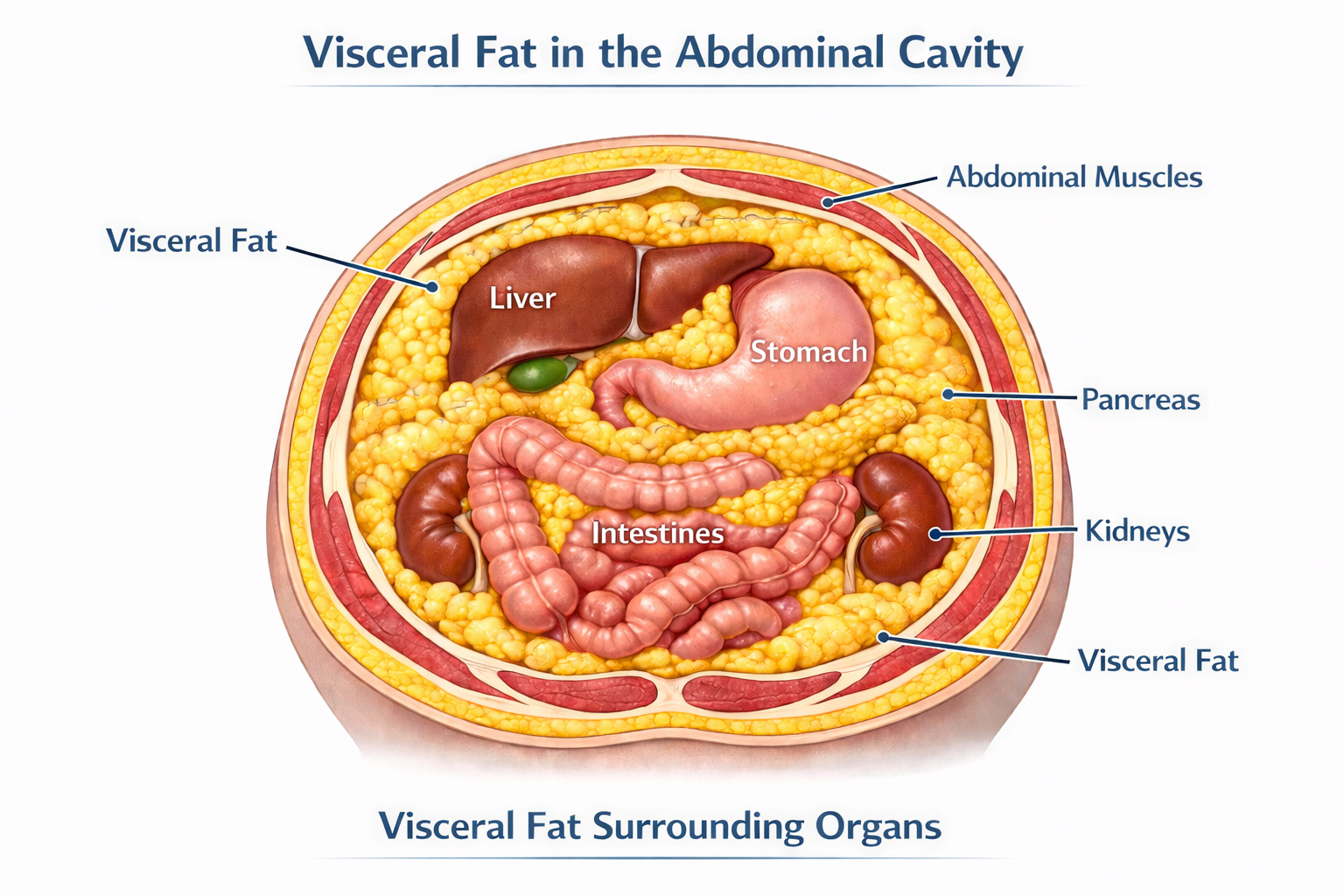
Visceral Fat Is a Hormone Problem — Not a Willpower Problem
If you're doing everything right and still carrying stubborn abdominal fat, the problem may not be discipline — it may be your hormones. Learn why visceral fat is a metabolic and hormonal problem, and how we assess and treat it at Precision Hormone Consulting.
If you've cleaned up your diet, started lifting weights, cut back on alcohol, and you're still carrying stubborn fat around your midsection — the frustration is understandable. Most people in that position assume they need to do more, or try harder. What they actually need is better information.
Abdominal fat is not simply the result of caloric excess or insufficient discipline. For a significant portion of people — particularly those in midlife — stubborn visceral fat is a hormonal and metabolic problem. It responds to hormonal and metabolic solutions. Understanding why requires a closer look at what visceral fat actually is.
Not All Body Fat Behaves the Same Way
The fat you can pinch just beneath the skin is called subcutaneous fat. It's not metabolically inert, but it's relatively benign compared to the fat that accumulates deep inside the abdominal cavity — surrounding the liver, pancreas, and intestines. That's visceral fat, and it behaves very differently.
Visceral adipose tissue is biologically active. It functions, in many respects, as an endocrine organ — secreting hormones, driving inflammation, and interfering with the metabolic systems that govern energy, appetite, and hormonal balance. The technical term for these secreted compounds is adipokines, and their effects ripple throughout the body.
When visceral fat is elevated, leptin — the hormone that signals satiety — becomes dysregulated, contributing to persistent hunger even in the context of adequate intake. Adiponectin, a hormone that improves insulin sensitivity and reduces inflammation, declines. Pro-inflammatory cytokines like TNF-α and IL-6 rise, creating a state of chronic low-grade systemic inflammation that quietly drives cardiovascular risk, metabolic dysfunction, and hormonal disruption.
Visceral fat is also rich in aromatase — an enzyme that converts androgens like testosterone into estrogens. This is not a minor detail. It means that excess visceral fat doesn't just accumulate as a downstream effect of hormonal imbalance; it actively worsens that imbalance, accelerating androgen breakdown and feeding back on the very hormonal systems that keep fat distribution and metabolism healthy.
Visceral fat doesn't just respond to hormone imbalance — it creates it.
The Hormones Driving Visceral Fat Accumulation
Visceral fat and hormonal dysfunction reinforce each other. Addressing one without the other is rarely sufficient. Here's what the evidence shows for each major hormone axis:
Testosterone
Low testosterone is both a cause and a consequence of visceral fat accumulation. Testosterone promotes lean muscle mass and healthy fat distribution. As levels decline — which happens gradually in both men and women with age — fat preferentially shifts toward the abdomen. That visceral fat then accelerates testosterone breakdown through aromatization, producing more estrogen and suppressing the signaling pathway between the brain and the gonads. The result is a self-reinforcing cycle that worsens over time without intervention.
Estradiol
In women, estradiol plays an underappreciated role in metabolic health. It promotes favorable fat distribution, supports insulin sensitivity, and reduces systemic inflammation. The decline of estradiol at perimenopause and menopause is one of the primary drivers of the visceral fat accumulation many women notice in their 40s and 50s — even without meaningful changes in diet or activity level. Restoring physiologic estradiol is a legitimate metabolic intervention, not merely a quality-of-life measure.
DHEA
DHEA is the most abundant circulating steroid hormone in the body, and it declines significantly with age. Low DHEA correlates with increased visceral adiposity, reduced insulin sensitivity, and an elevated inflammatory state. It receives less attention than testosterone or estradiol in mainstream medicine, but it's a meaningful part of a comprehensive hormonal assessment.
Thyroid — Specifically Free T3
Thyroid hormone drives thermogenesis, fat oxidation, and insulin sensitivity. The clinically relevant form is Free T3 — the metabolically active fraction. Many standard workups stop at TSH, missing patients whose Free T3 is suboptimal even when TSH appears normal. When Free T3 is low, the metabolic engine slows: fat oxidation decreases, insulin resistance worsens, and visceral fat accumulates even in patients doing everything else right.
Cortisol
Visceral adipocytes have a high concentration of glucocorticoid receptors, making them exquisitely responsive to cortisol — the body's primary stress hormone. Chronic psychological or physiological stress translates directly into central fat accumulation, elevated blood glucose, and worsening insulin resistance. Cortisol dysregulation isn't optional to address in any serious approach to metabolic health.
Insulin Resistance
Insulin resistance and visceral fat are so tightly intertwined that separating cause from consequence is often impossible. Visceral fat drives insulin resistance through adipokine dysregulation, chronic inflammation, and excess free fatty acid release into the portal circulation. Insulin resistance, in turn, creates a hormonal environment that favors further visceral fat accumulation. Addressing one without the other rarely produces durable results.
What We Measure — and Why It Matters
Identifying visceral fat burden and its downstream metabolic effects requires looking beyond a scale or a BMI table. BMI, in particular, tells you almost nothing about where fat is distributed or how metabolically active it is. Two people with identical BMIs can carry dramatically different metabolic risk.
At Precision Hormone Consulting, a comprehensive assessment includes:
Waist circumference and waist-to-hip ratio are simple but meaningful starting points — far more predictive of metabolic risk than weight or BMI alone. In-office, we use InBody bioelectrical impedance analysis to go further, generating a validated estimate of visceral fat, lean mass, and body composition that gives us a quantitative baseline and a way to track changes over time. The clinical gold standards for visceral fat measurement — DEXA and MRI — offer greater precision but are expensive and largely inaccessible outside of research settings. For the purposes of clinical monitoring, our combination of anthropometric measures and InBody analysis provides a practical, actionable picture of visceral fat burden without requiring a radiology referral.
Fasting insulin and HOMA-IR — the most direct available measures of insulin resistance. A fasting glucose in the normal range can mask significantly elevated insulin levels, which is where the metabolic damage is already occurring.
Triglyceride/HDL ratio — an accessible and underutilized surrogate for insulin resistance and small, dense LDL particle burden. A standard lipid panel showing normal total cholesterol can coexist with substantial cardiovascular risk in a patient with visceral adiposity and insulin resistance.
hs-CRP — high-sensitivity C-reactive protein, used as a marker of systemic low-grade inflammation driven by visceral fat.
Adiponectin — an inverse marker of visceral fat and insulin resistance. Low levels indicate significant metabolic risk even before glucose dysregulation becomes overt on a standard chemistry panel.
SHBG (Sex Hormone Binding Globulin) — low SHBG is a reliable early signal of hepatic insulin resistance, often appearing before other markers become abnormal. It is particularly useful in women as an early warning sign of metabolic dysfunction.
LH/FSH ratio — in reproductive-age women, normal physiology produces an FSH level approximately twice that of LH. When insulin resistance is present, this ratio begins to narrow — sometimes approaching 1:1 — even before other metabolic markers are overtly abnormal. This is an early, underutilized signal of insulin's effect on the hormonal axis, and it does not require a PCOS diagnosis to be clinically meaningful.
These markers, taken together, provide a far more complete picture of metabolic health than any single value.
The PHC Approach: Treating the Root Cause
A patient came to us in their mid-forties — lean by BMI standards, active, eating well. Their complaint was persistent abdominal fullness and fatigue that had been gradually worsening for two years. Standard labs from their primary care physician had come back normal. Our panel told a different story: suboptimal Free T3, low SHBG, an elevated fasting insulin consistent with early insulin resistance, and a testosterone level that was technically within the reference range but well below what we'd expect for their age and activity level. Within four months of a targeted protocol, their body composition had shifted meaningfully and their energy had returned.
That kind of presentation is common. The tools to identify and address it are available — they just aren't part of routine care.
Hormone Optimization
Restoring physiologic hormone levels is one of the most effective metabolic interventions available. Testosterone optimization in both men and women improves lean muscle mass, reduces visceral fat, and enhances insulin signaling. Estradiol replacement — particularly relevant around perimenopause and menopause — shifts fat distribution favorably and supports metabolic function. DHEA optimization reduces inflammation and supports body composition. Ensuring Free T3 is in an optimal range, not merely a "not flagged" range, restores the metabolic rate that drives fat oxidation.
Peptide Therapy
Growth hormone-releasing peptides are a valuable adjunct for patients with significant visceral fat burden. Tesamorelin has demonstrated specific efficacy in visceral fat reduction in clinical trials. CJC-1295/Ipamorelin combinations support broader growth hormone axis optimization, improving body composition, sleep quality, and recovery.
GLP-1 Medications
For patients with significant metabolic burden or insulin resistance, GLP-1 receptor agonists represent one of the most effective pharmacologic tools currently available. Their mechanisms go well beyond appetite suppression — they improve insulin signaling, reduce hepatic fat, lower systemic inflammation, and produce meaningful, sustained reductions in visceral adiposity.
It's worth noting that GLP-1 is itself a peptide hormone produced naturally in the gut. In patients with metabolic dysfunction, endogenous GLP-1 production is often impaired — meaning these medications are, in a meaningful sense, optimizing a hormone that the body is no longer producing adequately. That framing fits squarely within a hormone optimization model rather than a weight loss drug model.
Lifestyle Integration
No clinical protocol works in isolation. Resistance training, protein-adequate nutrition, quality sleep, and deliberate stress management all independently reduce visceral adiposity and improve insulin sensitivity. Our role is to help patients optimize the full picture — not simply prescribe and monitor. Clinical intervention amplifies the results of good lifestyle fundamentals; it doesn't replace them.
If You've Been Doing the Right Things and Still Not Getting Results
The frustration of doing everything by the book and still carrying stubborn abdominal fat is real — and it usually means something in the hormonal or metabolic picture hasn't been identified yet.
Visceral fat is not a character flaw. It is a metabolic and hormonal problem, and it responds to metabolic and hormonal solutions. The evidence is clear: optimizing testosterone, estradiol, DHEA, thyroid, and metabolic markers produces real, measurable improvements in body composition and long-term health outcomes.
At Precision Hormone Consulting, we specialize in exactly this kind of comprehensive, root-cause evaluation. If you're ready to understand what's actually driving your metabolic health — and address it systematically — we'd be glad to have that conversation.
Schedule a free consultation at precisionhormoneconsulting.com, or call the clinic to book an appointment. Virtual and in-person options are both available.
[DISCLAIMER] This content is for educational purposes only and does not constitute medical advice. Hormone optimization, peptide therapy, and GLP-1 medications involve prescription therapies that require individualized evaluation, monitoring, and ongoing clinical oversight. Some therapies discussed may be used off-label. Results vary. Consult a qualified physician before beginning any new treatment protocol.
Your Mitochondria May Be the Missing Piece: An Introduction to Methylene Blue
You're optimizing hormones, sleep, and nutrition — but something still feels off. The answer may be at the cellular level. A Texas physician explains what methylene blue actually does, who it's for, and why a 150-year-old compound is generating serious clinical interest again.
When You’re Doing Everything Right and Still Feel Wrong
You’re exercising consistently, sleeping reasonably well, eating a clean diet, and managing your hormones with the help of a knowledgeable provider. By most measures, you’re doing what you’re supposed to do. But there’s still something off — a persistent drag on your energy, brain fog that won’t fully clear, or a ceiling on your performance that no amount of lifestyle optimization seems to lift.
In many of these cases, the answer isn’t more optimization at the lifestyle level. It’s happening deeper — inside your cells, at the level of the mitochondria responsible for producing the energy that powers everything else. And there’s a compound with a 150-year track record in medicine that is increasingly being used to address exactly that problem.
It’s called methylene blue. It turns your urine blue. And it’s worth understanding.
What Is Methylene Blue, and Why Does It Have Such a Long History?
Methylene blue is a synthetic compound first developed in 1876 as an industrial dye — the same chemistry behind blue denim. Within a decade it was being used medically: first as a biological stain, then as the first synthetic antimalarial, then for urinary tract infections and psychiatric conditions. It has been formally registered with the FDA for over a century and is on the World Health Organization’s list of essential medications. Its two current FDA-approved indications are treatment of methemoglobinemia and use as a surgical visualization dye. Everything discussed in this post beyond those uses is off-label — applied based on emerging research, and best guided by a physician familiar with the literature. There are nearly 30,000 published studies on PubMed. It is not fringe. It is, however, underused in clinical practice — which is why most patients have never heard of it.
The Mechanism: What Methylene Blue Actually Does in the Body
Mitochondria generate ATP — the currency your body uses for virtually every biological process — through a series of protein complexes called the electron transport chain (ETC). When that chain is impaired, the downstream effects are broad: fatigue, cognitive fog, slow recovery, impaired cellular repair.
Methylene blue is a redox-active compound that can both accept and donate electrons. In dysfunctional mitochondria, it acts as an alternative electron carrier — stepping in to shuttle electrons past the problem areas and restore ATP production. Think of it as a detour around a blocked highway.
It also scavenges excess reactive oxygen species (ROS), the unstable molecules generated by dysfunctional mitochondria that damage cellular structures. That action is targeted directly at the mitochondria — meaningfully different from a general antioxidant supplement. And at a longer-term level, methylene blue has been shown to upregulate pathways involved in creating new mitochondria, activating PGC-1α and potentially sirtuins, the same longevity-associated proteins linked to exercise and caloric restriction.
The core of methylene blue’s value isn’t one specific condition. It’s the mitochondria — and mitochondrial health is foundational to energy, cognition, hormonal function, and recovery.
Where the Clinical Interest Is Concentrated
Given its mechanism, it’s not surprising that methylene blue is being studied and used across a range of conditions that share mitochondrial dysfunction as an underlying feature. A few areas where the evidence is most developed:
Brain Health and Cognitive Function
The brain is one of the most mitochondria-dense organs in the body, and it is acutely sensitive to disruptions in ATP production. Methylene blue crosses the blood-brain barrier readily, concentrating in neuronal mitochondria. Research has demonstrated increases in brain-derived neurotrophic factor (BDNF), improvements in memory consolidation — particularly fear extinction memory — and anti-apoptotic effects that protect neurons from stress-related damage. In psychiatry, it has a century-long history of use in mood disorders and has shown particular promise in bipolar disorder, including antidepressant and anxiolytic effects without triggering manic episodes.
Fatigue and Post-Viral Syndromes
Chronic fatigue — including the subset of patients dealing with long COVID sequelae — involves measurable mitochondrial impairment and a shift toward inefficient cellular energy metabolism. Methylene blue has been studied for its ability to counteract this metabolic shift, modulate the inflammatory signaling that drives persistent symptoms, and support recovery of normal energy production. Dosing in this context is typically low and titrated gradually.
Dysautonomia and POTS
In conditions characterized by dysregulated vascular tone — including POTS and certain presentations of dysautonomia — methylene blue’s ability to modulate nitric oxide signaling and restore vascular tone has drawn clinical interest. By inhibiting excess nitric oxide production, it can help blood vessels constrict appropriately, improving circulation and reducing orthostatic symptoms.
A Patient’s Experience
A patient in their mid-forties with Hashimoto’s thyroiditis, chronic fatigue, recurrent headaches, and exercise intolerance had thyroid labs being managed but continued to feel limited. After G6PD screening came back normal, methylene blue was added at 50mg daily.
At six months, fatigue and headaches had improved meaningfully and the patient was exercising regularly — something they had not been able to tolerate before. Thyroid antibodies, which had been elevated, normalized. By one year, the patient weaned off methylene blue; the improvements held. This kind of response isn’t guaranteed, but it reflects the pattern that draws providers toward methylene blue in complex, multi-system cases where standard approaches have plateaued.
Who Is a Reasonable Candidate — and Who Should Avoid It
Methylene blue is appropriate for some patients and contraindicated for others. A thoughtful workup before prescribing includes reviewing current medications and screening for specific conditions.
Absolute contraindications include pregnancy (methylene blue is teratogenic), breastfeeding, and G6PD deficiency. G6PD is a genetic enzyme deficiency that impairs the red blood cell’s ability to handle oxidative stress; in affected individuals, methylene blue can trigger hemolytic anemia. G6PD deficiency is more prevalent in people of African, Mediterranean, and South Asian descent, and enzyme levels should be checked before initiating therapy in any patient.
Methylene blue is a monoamine oxidase inhibitor (MAOI), which means it interacts with serotonergic medications — SSRIs, SNRIs, tricyclic antidepressants, and other MAOIs. The risk of serotonin syndrome in the literature is almost entirely associated with high-dose IV administration in surgical settings, not oral use at the doses used in functional medicine. That said, any patient on serotonergic medications warrants a careful, individualized discussion before starting.
Patients who are typically good candidates: those with unexplained fatigue that persists despite optimized hormones and lifestyle, cognitive complaints including brain fog or memory concerns, post-viral syndromes, dysautonomia, or complex multi-system presentations with a suspected mitochondrial component.
Dosing, Purity, and What to Expect
Dosing follows a low-and-slow approach. A typical starting point is 8–16 mg per day, titrated upward based on response — most protocols in this setting land between 15 and 50 mg daily. Purity matters significantly: industrial and chemical grades of methylene blue can contain heavy metals. We prescribe USP pharmaceutical-grade only, sourced through compounding pharmacies with third-party batch testing.
Our formulation pairs methylene blue with ascorbic acid, which improves absorption and moderates the blue urine discoloration — a predictable, harmless side effect worth mentioning upfront. Other dose-dependent side effects include mild nausea or GI discomfort, which typically resolve with dose adjustment. Monitoring begins with a baseline G6PD level and medication review, with follow-up labs tailored to the individual.
Is Methylene Blue Worth Exploring for You?
If you’ve done the foundational work — hormones, sleep, nutrition, exercise — and there’s still a ceiling you can’t break through, the answer may be at the cellular level. Methylene blue is one of the more interesting tools in functional medicine precisely because it addresses a root mechanism rather than a symptom. But like any prescription compound, it deserves a proper evaluation and individualized dosing, not a one-size approach.
At Precision Hormone Consulting, we take the time to understand the full picture before adding anything to a patient’s protocol. If you’re curious about whether methylene blue might be appropriate for you, we’re happy to have that conversation. Free consultations are available virtually — you can book online — or by calling the clinic to schedule in person. No commitment, just a conversation.
[DISCLAIMER]
This content is for educational purposes only and does not constitute medical advice. The use of methylene blue for indications beyond FDA-approved applications is off-label and should only be undertaken under the supervision of a licensed physician who can evaluate your individual health history, current medications, and appropriateness for therapy. Do not start, stop, or change any medication or supplement based on information in this post.
What Is Bioidentical Hormone Replacement Therapy — and Is It Right for You?
The term "bioidentical" gets used loosely — but the distinction from synthetic hormones is real and clinically significant. Here's what BHRT actually is, which hormones are involved, and how to think about whether it belongs in your care.
The term “bioidentical” gets used loosely, and that creates genuine confusion about whether bioidentical hormone replacement therapy (BHRT) is meaningfully different from conventional hormone therapy or just well-packaged marketing. It’s a fair question. BHRT is a legitimate clinical approach with a defined pharmacological basis and a growing body of supporting evidence — but it requires proper evaluation, individualized dosing, and ongoing monitoring to do responsibly. Here’s what it actually is, how the key hormones are used, and how to think about whether it belongs in your care.
What “Bioidentical” Actually Means — and Why It Matters
Bioidentical hormones are molecularly identical to those the human body produces. Bioidentical estradiol has the same chemical structure as the estradiol your ovaries make; bioidentical testosterone matches what your testes or adrenal glands produce. Conventional hormone therapies often use synthetic compounds that are structurally similar but not identical — medroxyprogesterone acetate and conjugated equine estrogens being the most familiar examples. These compounds bind hormone receptors, but in ways the body wasn’t designed for. That mismatch is what drives the risks and side effects associated with synthetic hormones: increased clotting risk, adverse cardiovascular effects, and elevated breast cancer risk.
The distinction is most clinically significant for progesterone. Synthetic progestins increase the risk of blood clots and breast cancer. Bioidentical progesterone does neither — evidence suggests it actively reduces breast cancer risk. Conflating the two has caused unnecessary confusion and led many women to avoid hormone therapy that could genuinely help them. Bioidentical hormones interact with receptors the way the body expects. That difference in mechanism is the difference in risk profile.
Synthetic hormones carry risks because they bind receptors in ways the body wasn’t designed for. Bioidentical hormones don’t carry those same risks — because the body is designed to receive them.
The Hormones — What They Do and How They’re Used
BHRT is a personalized protocol built around individual lab findings and symptoms, not a single prescription. The hormones most commonly addressed are the following.
Testosterone — Men
Testosterone peaks in the mid-twenties and declines roughly 1 to 2% per year after thirty. By the time most men seek evaluation, they’ve been living with the downstream effects for years: fatigue, reduced drive, difficulty maintaining muscle, increased abdominal fat, disrupted sleep, and diminished libido. Treatment is delivered as a topical cream or injection. Cream produces more stable day-to-day levels and generates higher DHT — the more potent androgen driving libido, muscle, and energy — but requires consistent daily application. Injections eliminate absorption variability and suit patients who prefer a less frequent routine, though levels fluctuate more between doses. The right choice depends on the patient’s lifestyle and clinical profile.
Testosterone — Women
Testosterone is produced by the ovaries and adrenal glands in women and plays a central role in energy, libido, cognitive function, muscle tone, and mood. Levels begin declining in a woman’s thirties — well before menopause — and falling testosterone and progesterone are often the earliest hormonal markers of perimenopause, appearing years before estradiol shifts significantly. Delivery is cream or injection, with the same tradeoffs as in men. Topical cream has the added benefit of addressing local vaginal symptoms — dryness, discomfort, reduced sensitivity — alongside systemic effects, making it particularly effective for women managing both dimensions of decline.
Estradiol
Estradiol decline drives the hot flashes and night sweats most people associate with menopause — though perimenopausal hot flashes are more often triggered by loss of inhibin, a hormone that begins declining years before estradiol does. Beyond vasomotor symptoms, estradiol affects bone density, cardiovascular protection, cognitive function, and sleep. Oral estradiol is generally preferred for its favorable impact on lipids and cardiovascular health. For women with elevated clotting risk, transdermal cream is the appropriate alternative. Patches are available on patient request but are not a primary recommendation due to less consistent absorption and the absence of the cardiovascular benefits seen with oral dosing.
Progesterone
Progesterone is often framed as relevant only for women with a uterus. That misses most of its clinical importance. It begins declining in the early-to-mid thirties and its effects extend well beyond uterine protection: sleep quality, anxiety, mood stability, bone strength, cardiovascular health, and protection against breast, uterine, and ovarian cancers — benefits that apply regardless of surgical history. Oral micronized progesterone is preferred; its mild sedative quality taken at night is frequently therapeutic. For patients sensitive to that effect, a rapid-dissolving sublingual tablet achieves equivalent blood levels with less sedation.
Thyroid
Standard levothyroxine provides T4 only, but T4 must convert to the active T3 form in peripheral tissues — a process that can be impaired even when TSH is normal. Desiccated thyroid extract (DTE), which contains both T4 and T3 in a physiologically relevant ratio, is the primary approach used here. Compounded T3/T4 combination therapy serves as an alternative when DTE isn’t the right fit. Both require careful titration and ongoing monitoring of Free T3 and Free T4.
No two patients look exactly alike. The protocol that works is the one built around your specific labs, symptoms, and history — not a standardized template.
Off-Label Use, Compounding, and Monitoring
Most bioidentical hormones used in BHRT are compounded by a licensed pharmacy, allowing for individualized dosing and delivery forms unavailable in standard commercial products. Compounded preparations are not FDA-approved as finished drug products, but the active ingredients are FDA-regulated and compounding pharmacies operate under state pharmacy board oversight. BHRT is off-label not because the hormones are unproven, but because the FDA approval pathway is designed for standardized products, not individualized therapy.
What this requires clinically is structured monitoring. Every protocol begins with a comprehensive baseline evaluation. Symptom check-ins follow every one to two months; labs run approximately every three months initially, then less frequently once stable. Contraindications — including hormone-sensitive cancers, certain clotting disorders, and uncontrolled cardiovascular disease — are evaluated individually before any therapy begins.
What This Looks Like in Practice
A 52-year-old postmenopausal patient came in after two years of managing hot flashes with over-the-counter supplements. She wasn’t sleeping, her energy and mental clarity had declined significantly, and she’d attributed it to aging. Her physician had offered a standard estrogen patch but hadn’t measured testosterone or progesterone.
Baseline labs showed low estradiol, undetectable testosterone, progesterone below any meaningful range, and a Free T3 at the low end of the reference interval despite a normal TSH. We built a protocol around oral estradiol, oral micronized progesterone, low-dose testosterone cream, and desiccated thyroid extract. Sleep improved substantially by month three. By month six to seven, her energy, cognitive clarity, and overall wellbeing were meaningfully restored — the result of a complete evaluation and a protocol built around her specific picture, not a template.
Is BHRT Right for You?
BHRT is worth exploring if you’re experiencing fatigue, cognitive fog, disrupted sleep, mood changes, loss of muscle tone, reduced libido, or poor recovery — and either haven’t had a comprehensive hormone evaluation or have been told your labs are normal without a deeper conversation. It’s also worth exploring if you’ve been on conventional hormone therapy and still don’t feel right. Synthetic and bioidentical hormones are not the same thing, and the distinction has real clinical implications. The starting point is always a thorough evaluation, not an assumption that treatment is indicated before the full picture is clear.
Start with a Conversation
If any of this resonates, a free consultation is a reasonable next step — not a commitment to anything, just an opportunity to talk through what you’re experiencing and whether a comprehensive evaluation makes sense. Virtual consultations are available through the Precision Hormone Consulting website. To schedule in person, call the clinic directly.
Medical Disclaimer: The content in this post is intended for general educational purposes only and does not constitute medical advice. It is not a substitute for professional medical evaluation, diagnosis, or treatment. Bioidentical hormone replacement therapy involves compounded and off-label medications that require individualized assessment, physician oversight, and ongoing monitoring. Hormone therapy is not appropriate for everyone. Contraindications exist and must be evaluated on an individual basis by a qualified healthcare provider. Always consult a physician regarding your specific symptoms, history, and treatment options before initiating any hormone therapy.
Why Your Labs Look Normal But You Feel Terrible
Your doctor says your labs are fine. So why do you still feel exhausted, foggy, and off? The problem isn't your results — it's what "normal" actually means, and what most standard panels never measure.
You asked your doctor to check your labs. Everything came back normal. Your TSH is fine. Your testosterone is in range. Your thyroid is “unremarkable.” And yet you’re exhausted by two in the afternoon, your motivation has flatlined, your sleep feels unrefreshing, and you can’t recover from workouts the way you used to. You’re doing the right things — exercising, watching what you eat, managing stress — and still feel like something is fundamentally off.
You’re not imagining it. The problem isn’t that your labs are normal. The problem is what “normal” actually means — and what your doctor’s standard panel may not be measuring at all.
“Normal” Is Not the Same as Optimal
This distinction sits at the core of the clinical framework I was trained in. Through Worldlink Medical — founded by Neal Rouzier, MD, one of the leading physicians in evidence-based hormone optimization — I trained directly in the protocols and diagnostic approach that underpin everything we do at Precision Hormone Consulting. The central premise is straightforward: reference ranges are not wellness targets.
Most reference ranges are built from a statistical cross-section of the population — one that includes a large number of people who are sedentary, metabolically compromised, and aging without any active health management. When a lab says your testosterone is “in range,” that range was calculated to include people who feel exactly the way you feel right now. It tells you whether you have a disease-level abnormality. It doesn’t tell you whether your levels support how you want to feel and function.
In functional medicine, we look at where your values fall within the range, not just whether they cleared the threshold. And we account for the fact that the same lab value can mean different things in different people. Lifetime exposure to environmental toxins and endocrine-disrupting chemicals can reduce hormone receptor sensitivity — meaning the hormone is present, but the cells aren’t responding to it effectively. One person may feel well at a given level; another may need a higher level to achieve the same result. Treatment has to be calibrated to the person, not just the number.
A number doesn’t have to be flagged to be the reason you feel the way you do. Optimal and normal are not synonyms.
The Tests That Matter — and the Ones Most Panels Skip
The standard panel most physicians order captures only a fraction of what’s relevant to how you feel. Here’s what a comprehensive evaluation actually looks at.
Testosterone — Total, Free, and SHBG
Total testosterone is the number most doctors report, but roughly 60% of it is bound to sex hormone-binding globulin (SHBG) and biologically inactive. Only the free fraction — typically 2 to 3% of the total — is available to act on tissues. Someone with a total testosterone of 550 ng/dL and high SHBG may have less usable hormone in circulation than someone with a total of 380 and normal SHBG. Without measuring free testosterone and SHBG together, you’re working from an incomplete picture.
Thyroid — TSH, Free T3, and Free T4
TSH is a pituitary signal, not a direct measure of thyroid output. Free T4 is what the thyroid secretes; Free T3 is the biologically active form tissues actually use. Conversion from T4 to T3 can be impaired by chronic stress, inflammation, and nutritional gaps — even when TSH and T4 are perfectly normal. A patient with poor T4-to-T3 conversion can have a textbook TSH and feel every symptom of hypothyroidism. You can’t see that without measuring Free T3 directly.
Cortisol and DHEA-S
Cortisol should peak in the early morning to drive waking energy and decline across the day. Disruptions to this rhythm often go undetected on a standard panel. AM cortisol measured alongside DHEA-S — an adrenal androgen that declines under chronic stress — gives a functional picture of adrenal output. Low-normal AM cortisol with suppressed DHEA-S correlates closely with the pattern many patients describe: dragging in the morning, wired at night, poor stress tolerance, and energy that never fully charges.
Estradiol, Progesterone, FSH, and LH
In women approaching or past menopause, declining estradiol contributes to sleep disruption, cognitive fog, joint discomfort, and mood changes that often get attributed to stress or aging. In men, estradiol is frequently overlooked despite its role in bone density, cardiovascular health, libido, and mood — both high and low levels cause symptoms that are easy to miss without measuring. FSH and LH clarify whether a hormonal deficiency is originating in the brain’s signaling or in the gonads themselves, which shapes the treatment approach.
IGF-1 and Metabolic Markers
IGF-1 reflects growth hormone activity and declines with age and poor sleep. Low levels correlate with impaired recovery, poor body composition, and reduced metabolic function — yet it rarely appears on standard panels. Alongside IGF-1, I look for early patterns of insulin resistance and visceral fat accumulation. Visceral fat is hormonally active tissue that drives systemic inflammation and oxidative stress, both of which impair mitochondrial function and create a state of cellular energy deficiency. This cascade underlies a significant portion of the fatigue, brain fog, and poor recovery that bring patients in — and it’s identifiable before it progresses to frank metabolic disease.
A standard panel is designed to rule out disease. A comprehensive evaluation is designed to explain symptoms — and those are fundamentally different goals.
What This Looks Like in Practice
A patient came to me in their mid-forties — active, eating well, getting adequate sleep by any conventional measure. Their primary care physician had run a metabolic panel, CBC, and TSH. Everything was normal.
What the panel hadn’t captured: free testosterone in the low-normal range, a Free T3 at the bottom of the reference interval, DHEA-S well below age expectation, and an AM cortisol suggesting the adrenal axis wasn’t delivering its morning output. No single number was flagged. Taken together, the picture was clear — and entirely consistent with how they described their days. Early changes in energy and sleep emerged within the first couple of months. Full symptom resolution took closer to eight months, which is typical.
Who Should Consider a Comprehensive Evaluation
This kind of evaluation makes sense if your standard labs came back clean but you’re still dealing with persistent fatigue, cognitive fog, disrupted sleep, low motivation, changes in body composition, or reduced exercise tolerance. It also makes sense if you’re in your late thirties or older and have noticed a meaningful decline in how you feel and recover over the past few years — even while doing everything right. If you’ve been told your levels are normal and the conversation stopped there, that’s worth revisiting.
What to Expect
We start with a comprehensive baseline panel, then monitor symptoms with check-ins every one to two months — how you’re sleeping, how your energy is tracking, how you’re recovering. Lab work runs approximately every three months in the early phase while levels are actively changing, then less frequently once you’re stable on a consistent protocol.
Meaningful symptom relief typically takes six to nine months. Hormone levels didn’t decline overnight, and correcting them too aggressively creates its own problems. Most patients notice early improvements in sleep and energy within four to eight weeks; body composition and overall resilience follow over the subsequent months. For some, addressing receptor sensitivity — through reducing toxic burden or tools like infrared sauna — is as important as the hormone level itself.
Start with a Conversation
If you’ve been told your labs are normal and you still don’t feel right, that’s worth exploring. A free consultation is a good first step — not a commitment to anything, just an opportunity to talk through what you’re experiencing and whether a comprehensive evaluation makes sense for you.
You can book a virtual consultation directly through the Precision Hormone Consulting website, or call the clinic to schedule in person. Dr. Wilcox is also listed as a featured physician on the Worldlink Medical provider directory — an independent resource for patients looking to verify credentials in evidence-based hormone optimization.
Further Reading
The clinical philosophy behind this practice is grounded in the work of Neal Rouzier, MD. His book Normal Isn’t Optimal is the foundational text for the Worldlink Medical training program and a useful primer for anyone who wants to understand the evidence base before their first consultation.
Medical Disclaimer: The content in this post is intended for general educational purposes only and does not constitute medical advice. It is not a substitute for professional medical evaluation, diagnosis, or treatment. Lab reference ranges and clinical interpretations vary depending on the individual, the laboratory, and the clinical context. Always consult a qualified healthcare provider regarding your specific symptoms, laboratory results, and treatment options. Hormone therapies discussed in this content may involve off-label use and require physician oversight, individualized assessment, and ongoing monitoring.
Sermorelin vs. Ipamorelin/CJC-1295 vs. Tesamorelin: Which Growth Hormone Peptide Is Right for You?
A physician's guide to the real differences between sermorelin, ipamorelin/CJC-1295, and tesamorelin — three distinct GHRH peptides with different mechanisms, potency, and ideal use cases. Written by Darrell Wilcox, MD.
Growth hormone output declines significantly with age — production can fall by more than half between your 20s and 60s. For many people, that decline shows up as stubborn body fat that won't budge, slower recovery from exercise, poor sleep, and a general sense that the body isn't responding the way it used to.
Peptide therapy is one way to address that decline. But the three most commonly prescribed options — sermorelin, ipamorelin/CJC-1295, and tesamorelin — are not interchangeable versions of the same treatment. Choosing between them should be based on your goals, not whoever marketed their option most aggressively.
What These Peptides Have in Common
None of these are synthetic human growth hormone (HGH). They are growth hormone-releasing hormone analogs that work by signaling your pituitary gland to produce its own GH — naturally, in pulses, through your body's existing feedback loops.
This matters. Synthetic HGH bypasses those feedback mechanisms entirely, which is why it carries risks like insulin resistance and soft tissue overgrowth. These peptides work with your body's regulatory systems, not around them.
All three drive the same downstream process: your pituitary releases GH → your liver produces IGF-1 → IGF-1 drives the benefits you're after: fat metabolism, tissue repair, sleep quality, and body composition improvements. The differences lie in how strongly each peptide stimulates that process, and through what mechanism.
The Three Options
Sermorelin — The Foundation
Sermorelin is the gentlest of the three. It's a fragment of the natural GHRH molecule, has decades of clinical use behind it, and produces a modest, dose-dependent increase in GH output.
Sleep quality is typically the first benefit patients notice, often within two to four weeks. Recovery between training sessions improves. Over three to six months, most patients see gradual improvements in skin elasticity, hair quality, and body composition.
Dosing is simple: one subcutaneous injection daily, typically before bed to align with your body's natural nighttime GH release. Side effects are generally mild — occasional water retention, temporary wrist or hand numbness, minor injection site irritation.
Best for people new to peptide therapy, those with broad wellness goals across sleep, recovery, and gradual body recomposition, and anyone who wants a simple daily protocol with a mild side effect profile.
Ipamorelin/CJC-1295 — The Middle Ground
This is a combination protocol, and the pairing is intentional. CJC-1295 is a GHRH analog that stimulates GH release through the same receptor pathway as sermorelin. Ipamorelin works through a completely different pathway — the ghrelin receptor — and is notable for its selectivity: unlike older secretagogues, it does not significantly raise cortisol or prolactin at therapeutic doses.
Together, they stimulate GH release through two separate mechanisms simultaneously, producing a more robust response than either would alone — and meaningfully stronger than sermorelin. In clinical practice, both are administered as a single combined daily subcutaneous injection, keeping the protocol simple while delivering the synergistic benefit of dual-pathway stimulation.
Sleep and recovery improvements are similar to sermorelin but often more pronounced. Body recomposition is more noticeable. Side effects are moderate — water retention and post-injection flushing are more common than with sermorelin, but cortisol and prolactin remain stable.
Best for patients who want a stronger GH response, those stepping up from sermorelin, and anyone seeking meaningful body recomposition alongside the broader wellness benefits.
Tesamorelin — The High-Intensity Option
Tesamorelin is the full-length GHRH molecule with a structural modification that makes it resistant to the enzyme that normally breaks it down quickly in the body. This gives it a longer duration of action and the most potent GH response of the three.
It is the only peptide in this group with FDA approval — specifically for reducing visceral fat, the dangerous fat that surrounds your internal organs, in a specific patient population. The clinical trials supporting that approval showed IGF-1 increases of 50–100% above baseline and approximately 15% reduction in visceral fat over 26 weeks, confirmed by CT imaging, along with improvements in triglycerides and related metabolic markers.
Dosing is typically daily, though a five-days-on, two-days-off schedule is commonly used in clinical practice to manage water retention. Side effects are the most pronounced of the three — water retention, carpal tunnel-like symptoms from fluid retention, and a small but measurable effect on glucose tolerance in some patients. Monitoring of IGF-1, fasting glucose, and HbA1c is essential throughout treatment.
Best for patients whose primary goal is visceral fat loss, already-fit individuals targeting stubborn midsection fat, and those who want the most aggressive body recomposition results and are prepared for careful monitoring.
A Patient Story
A patient in their late 40s came in frustrated. Consistent training for years, eating well, sleeping reasonably — and still couldn't move the midsection fat or recover the way they used to. Bloodwork was otherwise unremarkable. IGF-1 was in the lower third of the reference range.
We started with ipamorelin/CJC-1295. Within the first month, sleep improved noticeably. By month three, recovery between sessions had shortened and body composition had begun to shift. At six months, they were down several inches at the waist and training harder than they had in a decade.
No shortcuts. The peptide created a more favorable hormonal environment. Consistent training and nutrition did the rest.
How to Choose
Sermorelin is the right starting point if your goals span sleep, recovery, skin, energy, and gradual body composition improvement — or if you're new to injectable peptide therapy and want a gentle introduction. Mildest side effects, simplest daily protocol.
Ipamorelin/CJC-1295 is the step up. Choose this if you want a stronger GH response, more noticeable body recomposition, or if sermorelin didn't deliver the results you were after. Daily combined injection, moderate side effects, dual-pathway stimulation.
Tesamorelin is the high-intensity option. Choose this if visceral fat reduction is your primary goal, you're already doing the lifestyle fundamentals consistently, and you want the most aggressive protocol backed by the strongest clinical evidence. Requires diligent monitoring.
Many patients begin with sermorelin or ipamorelin/CJC-1295 and advance based on their response. Your physician should guide that sequence based on your labs and goals.
What to Expect
Results build progressively. Most patients notice improved sleep and energy within the first two to four weeks. Recovery improvements follow in the first one to three months. Meaningful body composition changes take three to six months of consistent use — don't evaluate results before that three-month mark.
All three protocols require regular monitoring: IGF-1 every three to six months, along with fasting glucose, HbA1c, and thyroid function. These are prescription medications that require physician oversight, not self-directed supplementation.
Ready to Find Out Which Protocol Fits You?
If any of this resonates, the next step is a conversation — not a commitment. At Precision Hormone Consulting, we offer free consultations to review your labs, understand your goals, and determine whether peptide therapy is appropriate and which protocol makes sense for your situation.
You can book a virtual consultation online or call us directly to schedule in person. Either way, you'll leave with a clear picture of where you stand and what your options are.
This article is for educational purposes only and does not constitute medical advice. Growth hormone peptides are prescription medications. Consult a licensed physician before beginning any peptide therapy protocol.